Download
1 / 25
250 likes | 517 Views

E N D
1. Community-Acquired Methicillin Resistant Staphylococcus Aureus in a Military Setting LCDR E. Rebecca Beal-Landis, MD
Naval Hospital Pensacola, FL
March 16, 2007
2. Objectives Definition of CA-MRSA
Transmission
Prevalence
Risk Factors
Diagnosis
Treatment
Decolonization
Prevention
3. CA-MRSA Staphyloccal bacteria that have become resistant to beta-lactam antibiotics.
Occurs in healthy persons without traditional MRSA associated risk factors.
Spectrum of disease similar to MSSA- mostly SSTIs and less commonly pneumonia, and sepsis. All MRSA strains share a transpeptidase Penicillin-binding protein 2a (PBP2a) which gives the organism the ability to restore cell wall biosynthesis in the presence of b-lactams.
MecA is carried on a mobile genetic element, the staphylococcal cassette chromosome (SCCmec). SCCmec encodes two recominases, which mediate excision and reintegration of mecA into the chromosome. There are four SCCmec types known. Hospital acquired MRSA carries SCCmec Type I, II, and III. CA-MRSA carries type IV SCCmec, which is smaller and may be able to transfer more easily.
CA-MRSA usually describes MRSA that began in the community. There is overlap and the Type IV SCCmec has been noted in both CA and H-MRSA.
Clusters of the same clone have been noted in separate outbreaks � HS wrestling team in Vermont, rugby team UK, intrafamily, in daycare nurseries, among Native Americans in Nebraska and Alaska, in Minnesota.
Pulsed field gel electrophoresis is the gold standard for typing, and identifies clones of common origins
Currently there are 5 clones of CA-MRSA circulating globally:
USA300: PVL (Panton-Valentine leukocidin)-positive isolates. PVL is a cytotoxin that lyses white blood cells and mediates tissue necrosis, is associated with necrotizing cutaneous infections, and encodes a virulence factor for primary skin infection and pneumonia. PVL cytotoxin production is characteristic of isolates causing severe hemorrhagic pneumonia. Panton and Valentine described leukocidin as a virulence factor on 1932. PVL toxin was correlated in France 1985-1998 with staphylococcal isolate submitted to a reference lab. 93% furunculosis isolate +; 85% cases of community onset pneumonia + (61% fatal, autopsies showed diffuse, bilateral necrotic hemorrhagic pneumonia).
All MRSA strains share a transpeptidase Penicillin-binding protein 2a (PBP2a) which gives the organism the ability to restore cell wall biosynthesis in the presence of b-lactams.
MecA is carried on a mobile genetic element, the staphylococcal cassette chromosome (SCCmec). SCCmec encodes two recominases, which mediate excision and reintegration of mecA into the chromosome. There are four SCCmec types known. Hospital acquired MRSA carries SCCmec Type I, II, and III. CA-MRSA carries type IV SCCmec, which is smaller and may be able to transfer more easily.
CA-MRSA usually describes MRSA that began in the community. There is overlap and the Type IV SCCmec has been noted in both CA and H-MRSA.
Clusters of the same clone have been noted in separate outbreaks � HS wrestling team in Vermont, rugby team UK, intrafamily, in daycare nurseries, among Native Americans in Nebraska and Alaska, in Minnesota.
Pulsed field gel electrophoresis is the gold standard for typing, and identifies clones of common origins
Currently there are 5 clones of CA-MRSA circulating globally:
USA300: PVL (Panton-Valentine leukocidin)-positive isolates. PVL is a cytotoxin that lyses white blood cells and mediates tissue necrosis, is associated with necrotizing cutaneous infections, and encodes a virulence factor for primary skin infection and pneumonia. PVL cytotoxin production is characteristic of isolates causing severe hemorrhagic pneumonia. Panton and Valentine described leukocidin as a virulence factor on 1932. PVL toxin was correlated in France 1985-1998 with staphylococcal isolate submitted to a reference lab. 93% furunculosis isolate +; 85% cases of community onset pneumonia + (61% fatal, autopsies showed diffuse, bilateral necrotic hemorrhagic pneumonia).
4. Transmission Direct person to person contact
Sharing of towels or personal hygiene items
Athletic equipment
Clothes
Drug use equipment
Contact sports
Food-borne
Nov 2000 MI State Prison outbreak: 59 cases (3000 prisoners). Nasal cultures showed 5% carrier rate among asymptomatic prisoners.
CDC investigation documented spread by close contact, most often through the hands of an infected or nasally colonized person. Of those with CA-MRSA, >30% had contact with other inmates who had wound-care dressings or changed dressings; 90% shared personal items that were potentially contaminated by wound drainage, 58% lanced their own or other inmates� boils with fingernails or tweezers.
For ca-MRSA patients in the community, one study showed close contacts to have a 53% carriage rate, with 76% genetic CA-MRSA concordance. 2001
Fencers � shared gym equipment and use of same sensor wire under clothing � standard infection control interventions eliminated further cases.(increased hand hygiene, showering with soap after every practice, covering cuts & abrasions until healed, laundering personal items after each use, cleaning or laundering shared athletic equipment such as pads or helmets, establishing a routine cleaning schedule for the sensor wires, seeing a health care provider for wounds that do not heal or appear infected.
Pennsylvania college football team outbreak; risk factors were skin trauma from turf burns and shaving and sharing of unwashed bath towels.
Clusters found also in wrestlers among different weight groups, suggesting mats as common transmission source.
Nov 2000 MI State Prison outbreak: 59 cases (3000 prisoners). Nasal cultures showed 5% carrier rate among asymptomatic prisoners.
CDC investigation documented spread by close contact, most often through the hands of an infected or nasally colonized person. Of those with CA-MRSA, >30% had contact with other inmates who had wound-care dressings or changed dressings; 90% shared personal items that were potentially contaminated by wound drainage, 58% lanced their own or other inmates� boils with fingernails or tweezers.
For ca-MRSA patients in the community, one study showed close contacts to have a 53% carriage rate, with 76% genetic CA-MRSA concordance. 2001
Fencers � shared gym equipment and use of same sensor wire under clothing � standard infection control interventions eliminated further cases.(increased hand hygiene, showering with soap after every practice, covering cuts & abrasions until healed, laundering personal items after each use, cleaning or laundering shared athletic equipment such as pads or helmets, establishing a routine cleaning schedule for the sensor wires, seeing a health care provider for wounds that do not heal or appear infected.
Pennsylvania college football team outbreak; risk factors were skin trauma from turf burns and shaving and sharing of unwashed bath towels.
Clusters found also in wrestlers among different weight groups, suggesting mats as common transmission source.
5. Prevalence Prevalence is increasing!! 57% of all staph isolates at NHP are MRSA!!!
Review your command�s antibiogram to assess prevalence in your community.
Review patient�s risk factors Prevalence is unknown, and varies in geographically from <1% of the population in Portugal and NYC to 13% in Sri Lanka and >80% among American Natives in Southwestern Alaska. Suspected to be 1-3% of the general population in the US.
In FMC, 52% of cultures positive for SA are MRSA; overall 58% of SA cultures at NHP.
Mar-Nov 2006 � 395/675 = 58% MRSA NHP (395/774 = 58% all wound cultures)
34/57 = 59% MRSA FP (34/70 = 49% all wound cultures)
Prevalence is unknown, and varies in geographically from <1% of the population in Portugal and NYC to 13% in Sri Lanka and >80% among American Natives in Southwestern Alaska. Suspected to be 1-3% of the general population in the US.
In FMC, 52% of cultures positive for SA are MRSA; overall 58% of SA cultures at NHP.
Mar-Nov 2006 � 395/675 = 58% MRSA NHP (395/774 = 58% all wound cultures)
34/57 = 59% MRSA FP (34/70 = 49% all wound cultures)
6. Community-Acquired or Military Risk Factors
Crowded living conditions (prisons, military facilities, homeless shelters)
Certain populations (Pacific Islanders, Alaskan Natives, Native Americans)
Contact sports (football, rugby, wrestling)
Men who have sex with men
Sharing of towels, athletic equipment, personal items
Poor personal hygiene
More and more, seeing cases in healthy young adults, where the common risk factor is more likely to be deficient hygiene.
Crowded living conditions � prisons, military facilities, homeless shelters
Contact sports � football, rugby, wrestling
Traditional risk factors for acquisition of CA-MRSA:
Immunocompromised � Diabetes Mellitus, COPD, Renal Insufficiency, on Dialysis, chronic heart disease, HIV positive, tobacco or alcohol abuse.
Exposed to H-MRSA in the last 12 months or so
Treated with outpatient antibiotics.
More and more, seeing cases in healthy young adults, where the common risk factor is more likely to be deficient hygiene.
Crowded living conditions � prisons, military facilities, homeless shelters
Contact sports � football, rugby, wrestling
Traditional risk factors for acquisition of CA-MRSA:
Immunocompromised � Diabetes Mellitus, COPD, Renal Insufficiency, on Dialysis, chronic heart disease, HIV positive, tobacco or alcohol abuse.
Exposed to H-MRSA in the last 12 months or so
Treated with outpatient antibiotics.
7. Hospital-Acquired or Traditional Risk Factors Recent hospitalization (within 1 year)
Recent surgery (inpatient or outpatient, within 1 year)
History of recurrent abscesses, folliculitis, furunculosis or other skin infections
History of recurrent skin infections in a close contact or household member
Laboratory confirmed case of MRSA in a close contact or household member
Long-term care facility residence or repeated contact with residents
Intravenous drug use
Indwelling catheters
Medical conditions (e.g., diabetes, HIV,
renal failure)
8. Spiders have gotten a very bad rap!!!Spiders have gotten a very bad rap!!!
9. Brown Recluse Spider Bites violin-shaped marking on its top
bite produces a mild stinging
local redness and intense pain within eight hours
fluid-filled blister forms at the site and then sloughs off to leave a deep enlarging ulcer
can have mild fever, rash, nausea and listlessness
10. Brown Recluse Spider Bites vs. CA- MRSA
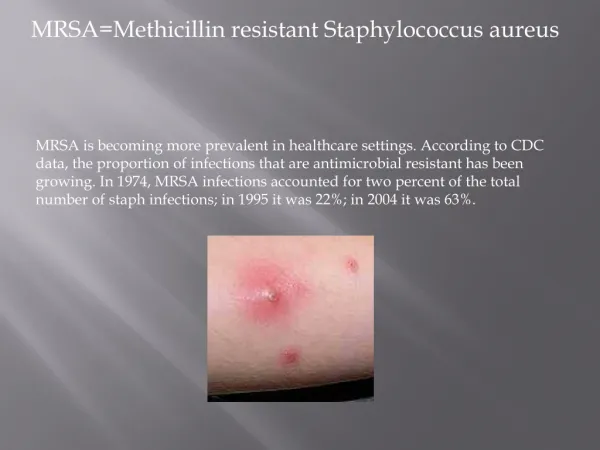
11. Diagnosis Commonly complain of infected pimples, spider bites, or sores.
Usually minor carbuncles, furuncles, abscesses.
Can be more extensive cellulitis, deep-seated abscesses, septic arthritis, pneumonia and sepsis.
Should be considered in the DDX of all military members with SSTIs.
Aerobic cultures should be obtained on all open lesions/ draining abscesses. Skin and soft tissue infection can become systemic and result in fulminate necrotizing hemorrhagic pneumonia
Case at NavHospPcola Jun 2006 � �spider bite� on neck treated with Dapsone, progressed to sepsis, MRSA Pneumonia
Case report Oakland CA 2005 � 31 yo male died within 53 hours of presentation to ER � sepsis, hemorrhagic pneumonia.
Overall 10 adult and 9 pediatric case reports of severe or lethal pneumonia due to ca-MRSA with the PVL gene
7 yo girl, infected hip joint; surgically drained, treated with cefazolin, changed to vancomycin when blood and joint cultures grew MRSA. Resp F; ARDS, pneumonia, empyema, died due to pulmonary hemorrhage 5 weeks later. No risk factors, no one in family with risk factors for MRSA.
16 mo girl died within 2 hours of arriving at hospital; 105.2, Seizures, petechial rash, irritable; blood cultures and csf grew MRSA; treated one month earlier with Amoxicillin for OM. No risk factors, no family risk factors.
13 yo girl F, hemoptysis, respiratory distress; prod cough, 2 cm papule on lower lip; CXR showed pleural effusion, lower lobe inifiltrate. Treated ceftriaxone, nafcillin, hypotensive in 5 hours, intubated, treated with vanc and cefotaxime but died 7th day. Blood, sputum, pleural fluid grew MRSA. No risk factors.
12 month boy with bronchiolitis, vomiting, dehydration, 105.2, petechial rash. CXR infiltrate c/w pneumonitis, developed pleural effusion, respiratory distress, hypotension, died second day. Pleural fluid MRSA. No risk factors. 2 year old sister had been treated 3 weeks earlier for a culture confirmed MRSA buttock infection. Isolates had identical antibiotic susceptibility profiles.
Bacteremia: 12% of pts with S. aureus bacteremia have infective endocaridtis � get TEE, consider ID consult.
Catheter-related Infections: TEE ; if no endocarditis, septic phlebitis, 14 days systemc abx. (Vanc)
Osteomyelitis: S. Aureus most commonly isolated microorganism in osteomyelitis; >1/3 may be MRSA. Hematogenous spread can lead to vertebral osteomyelitis, potentially epidural abcess formation. Tx: 4-6 weeks abx.
Joint Infections: S. Aureus is major pathogen. Drainage with 4 weeks abx. Last 2 weeks can be PO if not bacteremia.
Pulmonary Infections: pneumonia due to hematogenous spread or aspiration; S aureus ca pneumonia usually after influenza, community acquired pneumonia with PVL described.
CNS Infections: S aureus causes 2% all bacterial meningitis from hematogenous or post operative source. Usually had a shunt or an epidural catheter.
Skin and soft tissue infection can become systemic and result in fulminate necrotizing hemorrhagic pneumonia
Case at NavHospPcola Jun 2006 � �spider bite� on neck treated with Dapsone, progressed to sepsis, MRSA Pneumonia
Case report Oakland CA 2005 � 31 yo male died within 53 hours of presentation to ER � sepsis, hemorrhagic pneumonia.
Overall 10 adult and 9 pediatric case reports of severe or lethal pneumonia due to ca-MRSA with the PVL gene
7 yo girl, infected hip joint; surgically drained, treated with cefazolin, changed to vancomycin when blood and joint cultures grew MRSA. Resp F; ARDS, pneumonia, empyema, died due to pulmonary hemorrhage 5 weeks later. No risk factors, no one in family with risk factors for MRSA.
16 mo girl died within 2 hours of arriving at hospital; 105.2, Seizures, petechial rash, irritable; blood cultures and csf grew MRSA; treated one month earlier with Amoxicillin for OM. No risk factors, no family risk factors.
13 yo girl F, hemoptysis, respiratory distress; prod cough, 2 cm papule on lower lip; CXR showed pleural effusion, lower lobe inifiltrate. Treated ceftriaxone, nafcillin, hypotensive in 5 hours, intubated, treated with vanc and cefotaxime but died 7th day. Blood, sputum, pleural fluid grew MRSA. No risk factors.
12 month boy with bronchiolitis, vomiting, dehydration, 105.2, petechial rash. CXR infiltrate c/w pneumonitis, developed pleural effusion, respiratory distress, hypotension, died second day. Pleural fluid MRSA. No risk factors. 2 year old sister had been treated 3 weeks earlier for a culture confirmed MRSA buttock infection. Isolates had identical antibiotic susceptibility profiles.
Bacteremia: 12% of pts with S. aureus bacteremia have infective endocaridtis � get TEE, consider ID consult.
Catheter-related Infections: TEE ; if no endocarditis, septic phlebitis, 14 days systemc abx. (Vanc)
Osteomyelitis: S. Aureus most commonly isolated microorganism in osteomyelitis; >1/3 may be MRSA. Hematogenous spread can lead to vertebral osteomyelitis, potentially epidural abcess formation. Tx: 4-6 weeks abx.
Joint Infections: S. Aureus is major pathogen. Drainage with 4 weeks abx. Last 2 weeks can be PO if not bacteremia.
Pulmonary Infections: pneumonia due to hematogenous spread or aspiration; S aureus ca pneumonia usually after influenza, community acquired pneumonia with PVL described.
CNS Infections: S aureus causes 2% all bacterial meningitis from hematogenous or post operative source. Usually had a shunt or an epidural catheter.
12. CA-MRSA
13. CA-MRSA
14. CA-MRSA
15. CA-MRSA
16. CA-MRSA
17. Treatment Local incision and drainage and hot packs are the first-line therapies for skin infections.
Empiric Abx therapy
TMP-SMX 160mg/800mg bid x 10-14 days OR
Doxycycline/Minocycline 100mg bid x 10-14 days
Abx based on culture confirmation and sensitivity
Close follow-up in 24-48 hrs B lactams break down the cell wall.
Mupirocin inhibits protein synthesis by by reversibly binding bacterial isoleucyl transfer-RNA synthetase.
TMP and SMX inhibit sequential critical steps in bacterial synthesis of tetrahydrofolic acid � necessary cofactor in synthesis of bacterial DNA.
Hibiclens � Bactericidal
Hospitalized with CA-MRSA:
Vancomycin, Linezolid (Oxazolidinones, inhibits protein synthesis) - May have more penetration in lung tissue than Vancomycin and may be best for MRSA pneumonia. Avoid giving with SSRIs, CNS toxicity.
Daptomycin (Cubicin), cyclic liptopeptide; good for skin infections but poor lung penetration and inactivated by surfactant. Monitor CK during treatment if used. IV only.
B lactams break down the cell wall.
Mupirocin inhibits protein synthesis by by reversibly binding bacterial isoleucyl transfer-RNA synthetase.
TMP and SMX inhibit sequential critical steps in bacterial synthesis of tetrahydrofolic acid � necessary cofactor in synthesis of bacterial DNA.
Hibiclens � Bactericidal
Hospitalized with CA-MRSA:
Vancomycin, Linezolid (Oxazolidinones, inhibits protein synthesis) - May have more penetration in lung tissue than Vancomycin and may be best for MRSA pneumonia. Avoid giving with SSRIs, CNS toxicity.
Daptomycin (Cubicin), cyclic liptopeptide; good for skin infections but poor lung penetration and inactivated by surfactant. Monitor CK during treatment if used. IV only.
18. Treatment Do not use Clindamycin as empiric therapy, only use if susceptibility confirmed on culture and D tests negative.
Do not use Rifampin as monotherapy.
Potential life threatening toxicity
Drug interactions
Rifampin no longer recommended as adjuvant therapy unless discussed with infection control Resistance to flouroqinolones develops rapidly; erythromycin resistant strains can become resistant to Clindamycin.
We do the �D� test in the lab at NavHospPCOLA to determine Clindamycin sensitivity, however Clinda resistance 2003-4 NMC San Diego 79% vs 13% 2002; Clindamycin recommended only as last choice in empiric CA-MRSA treatment unless culture confirms organism is sensitive to Clinda. Rifampin no longer recommended except in consultation with NEPMU or ID staff (can be associated with Stevens-Johnson Syndrome, hemolysis, hepatitis, can decrease effectiveness of BCPs)
Clindamycin inhibits bacterial protein synthesis � binds 50S ribosomal subunit.
Quinolones bind bacterial DNA gyrase and topoisomerase IV � critical for DNA replication and repair.
Rifampin can result in potentially lifethreatening toxicity (e.g., Stevens-Johnson Syndrome, hemolysis with G6PD, pancreatitis, hepatitis, bone marrow suppression) and drug interactions (e.g., oral contraceptives) which preclude its recommendation. Use only after consultation with NEPMU or MTF staff.
Clindamycin and flouroquinolones now contraindicated as empiric therapy.
Clindamycin has increasing prevalence of resistance and concerns about inducible resistance, which prevents it from being recommended for the treatment of MRSA without confirmation that the isolate is sensitive. Many strains that are erythromycin-resistant confer inducible resistance to clindamycin. Some published studies estimate that 45% of staphylococcal isolates have inducible resistance. Use only after confirmation of sensitivity.
Fluoroquinolones are not recommended for the treatment of MRSA. Use only in conjunction with other medications (e.g., rifampin) and only after documentation of sensitivity.
Decolonization if 3 or more infections in < six months. Mupirocin BID for 10 days, Hibiclens wash daily for 5 days. Does not eradicate colonization, does not prevent recolonization, can result in mupirocin resistant strains.
Resistance to flouroqinolones develops rapidly; erythromycin resistant strains can become resistant to Clindamycin.
We do the �D� test in the lab at NavHospPCOLA to determine Clindamycin sensitivity, however Clinda resistance 2003-4 NMC San Diego 79% vs 13% 2002; Clindamycin recommended only as last choice in empiric CA-MRSA treatment unless culture confirms organism is sensitive to Clinda. Rifampin no longer recommended except in consultation with NEPMU or ID staff (can be associated with Stevens-Johnson Syndrome, hemolysis, hepatitis, can decrease effectiveness of BCPs)
Clindamycin inhibits bacterial protein synthesis � binds 50S ribosomal subunit.
Quinolones bind bacterial DNA gyrase and topoisomerase IV � critical for DNA replication and repair.
Rifampin can result in potentially lifethreatening toxicity (e.g., Stevens-Johnson Syndrome, hemolysis with G6PD, pancreatitis, hepatitis, bone marrow suppression) and drug interactions (e.g., oral contraceptives) which preclude its recommendation. Use only after consultation with NEPMU or MTF staff.
Clindamycin and flouroquinolones now contraindicated as empiric therapy.
Clindamycin has increasing prevalence of resistance and concerns about inducible resistance, which prevents it from being recommended for the treatment of MRSA without confirmation that the isolate is sensitive. Many strains that are erythromycin-resistant confer inducible resistance to clindamycin. Some published studies estimate that 45% of staphylococcal isolates have inducible resistance. Use only after confirmation of sensitivity.
Fluoroquinolones are not recommended for the treatment of MRSA. Use only in conjunction with other medications (e.g., rifampin) and only after documentation of sensitivity.
Decolonization if 3 or more infections in < six months. Mupirocin BID for 10 days, Hibiclens wash daily for 5 days. Does not eradicate colonization, does not prevent recolonization, can result in mupirocin resistant strains.
19. Decolonization Insufficient evidence to support use of topical or systemic antimicrobial therapy for eradicating MRSA colonization.
Cochrane review of 6 trials with 384 participants
Insufficient evidence to support the use of either topical or systemic
Potential for serious adverse events and development of antimicrobial resistance
Per CDC and NEHC, it maybe reasonable when pt has multiple documented recurrences.
Per NEHC consider Hibiclens washes from neck down x 5 days.
Cochrane review of 6 trials showed insufficient evidence to support the use of topical or systemic antimicrobial therapy for eradication of nasal or extra-nasal MRSA. No superiority of either topical or systemic therapy, or of combinations of these agents. Potentially serious adverse events and development of antimicrobial resistance may develop. Cochrane review of 6 trials showed insufficient evidence to support the use of topical or systemic antimicrobial therapy for eradication of nasal or extra-nasal MRSA. No superiority of either topical or systemic therapy, or of combinations of these agents. Potentially serious adverse events and development of antimicrobial resistance may develop.
21. Prevention- Education Provide information on transmission, prevention, treatment, and containment of MRSA infections.
Instructors and senior staff should receive training on recognition of suspicious wounds.
Encourage personnel to report all skin lesions to their supervisors or medical personnel.
23. Prevention- Hand hygiene program Periodic education given to recruits and staff on importance of hand hygiene and techniques.
ALL personnel should wash their hands with soap and running water for at least 15 seconds a minimum of 5 times per day. Daily showers.
Commands should ensure availability of liquid soap and water.
Use of hand sanitizers for times when running water not available.
25. Prevention- Eliminate sources of transmission Discourage sharing of towels, razors, brushes, etc.
Routine cleaning or laundering of athletic and training equipment
Routine disinfection of countertops, exam tables or other treatable surfaces.
All open wounds should be covered.
26. Questions???