Download
1 / 31
310 likes | 785 Views
Skin lesions in barracks: consider community-acquired methicillin-resistant Staphylococcus aureus infection instead of spider bites. Benedict Pagac CHPPM-North, Fort Meade, MD Richard Vetter Dept. of Entomology, University of California Riverside, CA Ronald Reiland MEDDAC, Fort Lee, VA

E N D
Skin lesions in barracks: consider community-acquired methicillin-resistant Staphylococcus aureus infection instead of spider bites Benedict Pagac CHPPM-North, Fort Meade, MD Richard Vetter Dept. of Entomology, University of California Riverside, CA Ronald Reiland MEDDAC, Fort Lee, VA D. Bolesh MEDDAC, Fort Lee, VA D. Swanson Dept. of Dermatology, Mayo Clinic, Scottsdale, AZ
ACKNOWLEDGEMENTS: CPT Aaron Miaullis, CHPPM PAC 1LT F. Priest, KAHC-Fort Lee, VA CPT Peters, KAHC-Fort Lee, VA Ms. S. Bokenko, KAHC-Fort Lee, VA MAJ Kevin Smith, KAHC-Fort Lee, VA Mr. Mills, EMO, Fort Lee, VA LTC Patrician Malley, KAHC-Fort Lee, VA CPT Kelly, KAHC-Fort Lee, VA Mr. Abdul Sheikh, DPW, APG, MD Mr. Ronald Purvis, DPW, Fort Myer, VA Mr. Kevin Faye, DPW, Fort Meade, MD LT Amber Hayden, PVNTMED, USMA, NY MAJ Trent Talbert, DTHC, Ft. McNair, Wash. DC SSG Crawford-Adams, KUSAHC, APG, MD Mr. Karl Neidhardt, CHPPM-North, FGGM, MD MAJ Samuel Jang, CHPPM, APG, MD CPT Andrew Plummer, CHPPM, APG, MD Ms. Nikki Jordan, CHPPM, APG, MD Mr. James Patrick, MACH, Ft. Benning, GA Mr. Richard Townsend, MACH, Ft. Benning, GA COL William Corr, MACH, Ft. Benning, GA Mr. Anthony Diederich, MACH, Ft. Benning, GA Mr. Robert Pawloski, MACH, Ft. Benning, GA MAJ Darlene Burns, MACH, Ft. Benning, GA Mr. Denny Kuhr, CHPPM-W, Ft. McPhereson, GA Mr. Derrick Pehlman, ILNG, Camp Lincoln, IL Mr. Adam Clemens, ILNG, Camp Lincoln, IL
Introduction • Fall, 2004 - DC Installation DPW pest management requests CHPPM assistance for “Brown Recluse bites in barracks” • DPW were “highly encouraged” to spray for the problem • 4-member inspection team examined interior and exterior of building for spider evidence and contributing factors • One of the six “bite” patients was available and allowed photograph of lesion • Consult with R. Vetter, UC Riverside spider specialist suggested CA-MRSA • Follow-up CA-MRSA culture of one patient was inconclusive • Revisted previous reports of multiple mysterious bites in barracks (e.g., NJ Army installation in 2003)
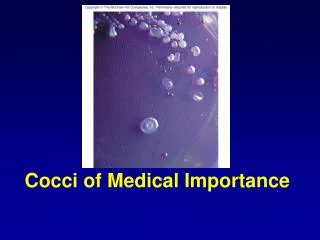
Results • No arthropods of confirmed medical importance were found in barracks at 7 military installations having reports of a spider bite problem. • At Fort Lee, lesions were documented in at least 23 personnel, from which confirmation of CA-MRSA was made in two barracks residents who were room mates. • In one example (Fort McNair) at least 80 manhours were expended for survey and control of a non-existent medical pest problem. • Operators at a minimum of four installations applied pesticides (e.g., permethrin), even though no medically important arthropods were present. • At Fort McNair, an orbweaver spider (Neoscona, Araneidae) was found. ( of no medical importance). • False spider reports persisted at one facility, even if education/awareness was previously established (due to turnover of medical and other authorities).
Results - continued Spider/Arthropod Investigations * Also see investigation, spring 1997 (MSMR, June 1997), Authors: N.A. Nee, et. al. ** See Poster: “Community Acquired MRSA; Fort Benning, Georgia, January 2001 – March 2005” Authors: Nikki Jordan, CPT Andrew Plummer, MAJ Sam Jang, James Patrick, MAJ Darlene Burns
Methods – Spider Survey Questions: What are the building number(s), Room number(s) of patients? How many patients? (contact information). Have patients seen a doctor? (name?). Was the lesion cultured for CA-MRSA? Did doctor say it was a spider bite, or did the patient suggest it? Did the Doctor or patient say that it was a “Brown Recluse Bite?” When did each of the patients first notice lesion or bite? Did the patient remember the actual moment of the bite, or did they wake up, or otherwise notice the lesion. Describe the bite. Are there 2-puncture (fang) holes in lesion? (sometimes, but not always visible) Did the patient actually see a spider? Are there any spiders present in the rooms/areas? (collect if available) Was the patient previously in a region/area known to be infested by spiders or Brown Recluse Spiders? Is there any spider webbing in rooms? (check corners, both at floor and ceiling level) Are there dropped ceilings in the patient’s rooms? Were the areas above dropped ceilings examined? (look for spiders or webbing, or, dead insects) Are there any sanitation issues noted? Is equipment that normally would be outdoors (e.g., ruck, boots, tents, tarps) stored in near patients room? Are window screens present? Are there gaps under exterior doors that permit entry by crawling insects/spiders? Are there other dead insects (e.g., on windowsills?) which would serve as prey for spiders? Did the exterior of the building have any attractive features or harborage? (e.g., lighting that attracts insects that, in turn, attracts spider predators). Do the patients use work-out equipment at the same location? Do the patients share a break room or reside in the same room?
Methods – Spider Survey Tools: Flashlight Sticky traps [note, mark dates on them, use a lot (at least 5-10 per average room), place them in secluded, dark places at floor/wall interface, check them after 3 days and at least weekly afterward). Digital Camera (to photograph rooms, potential contributing factors, insects, spiders, and the patient’s lesion (if given permission). Collection Vials (to use anything captured) Collection Vials (to give to occupants) Ladder (to access dropped ceiling) Portable vacuum (most valuable spider tool) Magnifying glass (to look at lesion as well as spider/insects)
What is CA-MRSA? • Methicillin-resistant Staphylococcus aureus is an emerging cause of skin and soft-tissue infections due to increased resistance of the bacteria to antibiotics. • In the last half-decade it has become more commonplace in the community (i.e., CA-), whereas before it was mainly associated with health-care settings. • Most infections are mild, but some advance to more serious systemic infection, bacteremia, and death. • Reported from sports participants, jail inmates, and children. • Some predisposing risk factors: close skin-to-skin contact, close person-person proximity, contaminated environment, suboptimal hand and personal hygiene, roommate with skin infection, familiy members working in health care, and conditions that may predispose to breaches in skin integrity such as harsh physical activity.
Discussion - continued Evidence supporting a non-spider causeespecially CA-MRSA Close-quartered living Multiple lesions on one individual Multiple individuals with lesions No spider Not in Brown Recluse range
Discussion - continued The Brown Recluse
- rufescens Courtesy - Rick Vetter
This young woman experienced a stinging sensation on her thigh while cleaning the basement in the early spring. An itchy red urticarial plaque was followed by central crusting 6-8 hours later. The next morning she developed a painful central necrotic ulcer. She was treated with oral dapsone, and the ulcer healed with minimal scarring 3 weeks later..
Those evil recluses…… • One floor: 597 Recluses • (88 days X 176 traps = 15,488 trap/nights) • Extrapolate: 3 floors X 597 = 1,791 Recluses • So, > 2,000 Recluses, 3 month period • How many confirmed bites per year? • Hundreds? • Dozens? • < 2 per year (ave)
oo oo oo o o o o oo oo
2 New Papers…. • Bites of Brown Recluse Spiders and Suspected Necrotic Arachnidism (Swanson & Vetter, New England Journal of Medicine, February 16 2005) • Arachnids Submitted as Suspected Brown Recluse Spiders (Araneae: Sicariidae): Loxosceles Spiders are Virtually Restricted to Their Known Distributions but Are Perceived to Exist Throughout the United States. (Vetter, Journal of Medical Entomology, July 2005)
Major points • Recluse bites are typically self-limited and self-healing, without long-term consequences. • There is not good evidence that other N. American spiders can cause necrosis [e.g., wolf, crab, yellow sac, (hobo?)] • No commercially available test exists to identify spider venom in wounds. • Other things cause conditions frequently misdiagnosed as brown recluse bites: e.g., staph, strep, herpes, diabetic ulcer, fungal infection, pyoderma gangrenosum, lymphomatoid papulosis, chemical burn, erythemas, Lyme disease, squamous-cell carcinoma, and much more… • Physicians should be skeptical of any undocumented history of a spider bite. • There is no therapy with proven efficacy for loxoscelism. Best approach – conservative simple first aid and local wound care.
Major points • The Brown Recluse Challenge: 2000-2005, UCR website – identify any spider submitted from U.S. that was perceived to be a brown recluse. • Results: 1,773 arachnids submitted from 49 states; 324 recluses from 15 states – all but four specimens were submitted from states historically considered to be within known distribution. • Recluses are rare in nonendemic areas, translocation unproven, and <10 infestations outside endemic range, generally restricted to 1 building.) • Recluses are limited in their dispersal potential.
Conclusions • CA-MRSA infections in barracks are becoming a common phenomenon in the NE. • It is probable that CA-MRSA is the causative agent when dealing with multiple patients with lesions and patients with multiple lesions, living in the same barracks, with no spider evidence. • It is highly improbable that a brown recluse spider would be responsible for a necrotic lesion in areas outside the recluse range. • Even in heavy recluse infestations, bites are infrequent. • True spider bites on the whole are not as common as believed or as medically diagnosed.