Download
1 / 62
660 likes | 1.28k Views
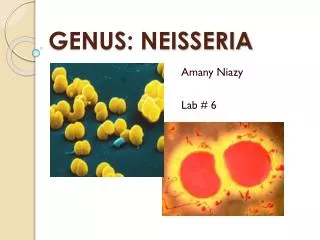
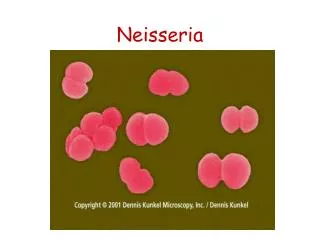
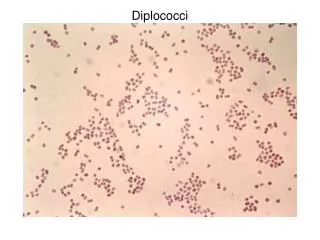
Neisseria. General Characteristics of Neisseria spp. Aerobic Gram-negative cocci often arranged in pairs ( diplococci ) with adjacent sides flattened (like coffe beans) Oxidase positive Most catalase positive Nonmotile Acid from oxidation of carbohydrates, not from fermentation.

E N D
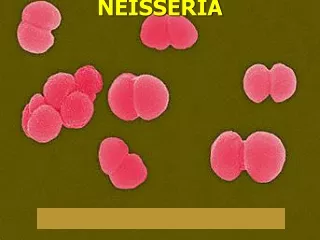
General Characteristics of Neisseria spp. • Aerobic • Gram-negative cocci often arranged in pairs (diplococci) with adjacent sides flattened (like coffe beans) • Oxidase positive • Most catalase positive • Nonmotile • Acid from oxidation of carbohydrates, not from fermentation
Important Human Pathogens Neisseria gonorrhoeae Neisseria meningitidis Other species normally colonize mucosal surfaces of oropharynx and nasopharynx and occasionally anogenital mucosal membranes
Neisseria Associated Diseases (ophthalmia neonatorum)
Differential Characteristics of Commonly Isolated Neisseria spp.
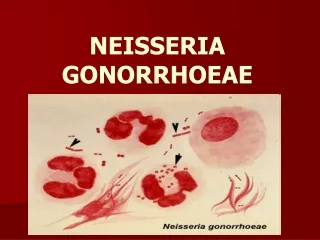
Neisseria gonorrhoeae (gonococcus)
General Overview of Neisseria gonorrhoeae • Readily transmitted by sexual contact • Gram-negative diplococci flattened along the adjoining side • Fastidious, capnophilic and susceptible to cool temperatures, drying and fatty acids • Requires complex media pre-warmed to 35-37C • Soluble starch added to neutralize fatty acid toxicity • Grow best in moist atmosphere supplemented with CO2 • Produce acid from glucose, but not from other sugars
Epidemiology of Gonorrhea • Seriously underreported sexually-transmitted disease • 350,000 reported cases in USA in 1998 • Down from 700,00 cases in 1990 • Found only in humans with strikingly different epidemiological presentations for females and males • Asymptomatic carriage is major reservoir • Transmission primarily by sexual contact • Lack of protective immunity and therefore reinfection, partly due to antigenic diversity of strains • Higher risk of disseminated disease in patients with late complement deficiencies
Differences Between Men & Women with Gonorrhea • IN MEN: • Urethritis; Epididymitis • Most infections among men are acute and symptomatic with purulent discharge & dysuria (painful urination) after 2-5 day incubation period • Male host seeks treatment early preventing serious sequelae, but not soon enough to prevent transmission to other sex partners • The two bacterial agents primarily responsible for urethritis among men are N. gonorrhoeae and Chlamydia trachomatis
Differences Between Men & Women with Gonorrhea (cont.) • IN WOMEN: • Cervicitis; Vaginitis; Pelvic Inflammatory Disease(PID);Disseminated Gonococcal Infection(DGI) • Women often asymptomatic or have atypical indications (subtle, unrecognized S/S); Often untreated until PID complications develop • Pelvic Inflammatory Disease (PID) • May also be asymptomatic, but difficult diagnosis accounts for many false negatives • Can cause scarring of fallopian tubes leading to infertility or ectopic pregnancy
Differences Between Men & Women with Gonorrhea (cont.) IN WOMEN (cont.): • Disseminated Gonococcal Infection (DGI): • Result of gonococcal bacteremia • Often skin lesions • Petechiae (small, purplish, hemorrhagic spots) • Pustules on extremities • Arthralgias (pain in joints) • Tenosynovitis (inflammation of tendon sheath) • Septic arthritis • Occasional complications: Hepatitis; Rarely endocarditis or meningitis
Pathogenesis of Neisseria gonorrhoeae • Fimbriated cells attach to intact mucus membrane epithelium • Capacity to invade intact mucus membranes or skin with abrasions • Adherence to mucosal epithelium • Penetration into and multiplication before passing through mucosal epithelial cells • Establish infection in the sub-epithelial layer • Most common sites of inoculation: • Cervix (cervicitis) or vagina in the female • Urethra (urethritis) or penis in the male
Gonococcal Virulence Factors • Antiphagocytic capsule-like negative surface charge • Only fimbriated (piliated) cells (formerly known as colony types T1 & T2) are virulent • Outer membrane proteins (formerly Proteins I, II, & III) • Por (porin protein) prevents phagolysosome fusion following phagocytosis and thereby promotes intracellular survival • Opa (opacity protein) mediates firm attachment to epithelial cells and subsequent invasion into cells • Rmp (reduction-modifiable protein) protects other surface antigens from bactericidal antibodies (Por protein, LOS) • Acquisition of iron mediated through Tbp 1 and Tbp 2 (transferrin-binding proteins), Lbp (lactoferrin binding protein) & Hbp (hemoglobin-binding protein)
GonococcalVirulence Factors (cont.) • Llipooligosaccharide (LOS) (Lipid A plus core polysaccharide but no O-somatic antigen polysaccharide side chain) has endotoxin activity • IgA1 protease • Acquisition in last two decades of two types of antibiotic resistance: • Plasmid-encoded beta-lactamase production • Chromosomally-mediated changes in cellular permeability inhibit entry of penicillins, tetracycline, erythromycin, aminoglycosides
Laboratory Characterization • Small, gram-negative diplococci in presence of polymorphonuclear leukocytes (PMN’s) seen microscopically in purulenturethral discharge • Susceptible to drying and cooling, so immediate culture of specimen onto pre-warmed selective (e.g., modified Thayer-Martin, Martin-Lewis agars) and non-selective media (chocolate blood agar) with moist atmosphere containing 5% carbon dioxide • Some strains inhibited by vancomycin (in many selective agars) and toxic substances like fatty acids and trace metals in protein hydrolysates and agar found in nonselective media • Five morphologically distinct colony types (formerly T1 through T5) that can undergo phase transition are no longer considered to be a useful distinction
Prevention & Treatment • Penicillin no longer drug of choice due to: • Continuing rise in the MIC • Plasmid-encoded beta-lactamase production • Chromosomally-mediated resistance • Uncomplicated infxn: ceftriaxone, cefixime or fluoroquinolone • Combined with doxycycline or azithromycin for dual infections with Chlamydia • Chemoprophylaxis of newborns against opthalmia neonatorum with 1% silver nitrate, 1% tetracycline, or 0.5% erythromycin eye ointments • Treatment of newborns with opthalmia neonatorum with ceftriaxone • Measures to limit epidemic include education, aggressive detection, and follow-up screening of sexual partners, use of condoms or spermicides with nonoxynol 9
Analytic Performance of Different Laboratory Detection Methods for Nesseria gonorrhoeae NOTE: Importance ofSensitivity vs. Specificityfor any Diagnostic Test
See Handout on Sensitivity & Specificity of Diagnostic Tests (Next two slides)
Analytic Performance of a Diagnostic Test (cont.) • Sensitivity = Measure of True Positive Rate (TPR) • = No. of True Pos. = No. of True Pos. = 80 = 80% • No. of Actual Pos. No. of (True Pos. + False Neg.) 80+20 Sensitivity • In conditional probability terms, the probability of a positive test given an actual positive sample/patient. • Specificity = Measure of True Negative Rate (TNR) • = No. of True Neg. = No. of True Neg. = 75 = 75% • No. of Actual Neg. No. of (True Neg. + False Pos.) 75+25 Specificity • In conditional probability terms, the probability of a negative test given an actual negative sample/patient.
Neisseria meningitidis (meningococcus)
General Overview of Neisseria meningitidis • Encapsulated small, gram-negative diplococci • Second most common cause (behind S. pneumoniae) of community-acquired meningitis in previously healthy adults; swift progression from good health to life-threatening disease • Pathogenicity: • Pili-mediated, receptor-specific colonization of nonciliated cells of nasopharynx • Antiphagocytic polysaccharide capsule allows systemic spread in absence of specific immunity • Toxic effects mediated by hyperproduction of lipooligosaccharide • Serogroups A, B, C, Y, W135 account for about 90% of all infections
Diseases Associated with Neisseria meningitidis • Following dissemination of virulent organisms from the nasopharynx: • Meningitis • Septicemia (meningococcemia) with or without meningitis • Meningoencephalitis • Pneumonia • Arthritis • Urethritis
Epidemiology of Meningococcal Disease • Humans only natural hosts • Person-to-person transmission by aerosolization of respiratory tract secretions in crowded conditions • Close contact with infectious person (e.g., family members, day care centers, military barracks, prisons, and other institutional settings) • Highest incidence in children younger than 5 years and particularly those younger than 1 year of age as passive maternal antibody declines and as infants immune system matures • Commonly colonize nasopharynx of healthy individuals; highest oral and nasopharyngeal carriage rates in school-age children, young adults and lower socioeconomic groups
Age Distribution of Meningococcal Disease in USA Lacking maternal antibody
Pathogenesis of Meningococcal Disease • Specific receptors (GD1 ganglioside) for bacterial fimbriae on nonciliated columnar epithelialcells in nasopharynx of host • Organisms are internalized into phagocytic vacuoles, avoid intracellular killing in absence of humoral immunity and complement system (patients with late complement deficiencies are particularly at risk) • Replicate intracellularly and migrate to subepithelial space where excess membrane fragments are released • Hyperproduction of endotoxin (lipid A of LOS) and blebbing into surrounding environment (e.g., subepithelial spaces, bloodstream) mediates most clinical manifestations including diffuse vascular damage (e.g., endothelial damage, vasculitis (inflammation of vessel walls), thrombosis (clotting), disseminated intravascular coagulation (DIC)
Skin Lesions of Meningococcemia NOTE:Petechiae have coalesced into hemorrhagic bullae.
Immunogenicity of Neisseria meningitidis • Following colonization of the nasopharynx, protective humoral immunity develops against the same or closely related organisms of the same serogroup, but not against other serogroups • Bactericidal activity of the complement system is required for clearance of the organisms • Cross-reactive protective immunity acquired with colonization by closely related antigenic strains and with normal flora of other genera (e.g., E. coli K1); progressive disease can occur in absence of serogroup-specific immunity
Laboratory Characterization of Neisseria meningitidis • Large numbers (e.g., >107cells/ml) of encapsulated, small, gram-negative diplococci (flattened along adjoining side) and polymorphonuclear leukocytes (PMN’s) can be seen microscopically in cerebrospinal fluid (CSF) • Transparent, non-pigmented nonhemolytic colonies on chocolate blood agar with enhanced growth in moist atmosphere with 5% CO2 • Oxidase-positive • Acid production from glucose and maltose but not from other sugars
Prevention and Treatment of Meningococcal Disease • Penicillin is drug of choice for treatment in adjunct with supportive therapy for meningeal symptoms • Increasing MIC mediated by genetic alteration of target penicillin binding proteins is being monitored) • Chloramphenicol or cephalosporins as alternatives • Chemoprophylaxis of close contacts with rifampin or sulfadiazine (if susceptible) • Polyvalent vaccine containing serogroups A, C, Y, and W135 is effective in people older than 2 years of age for immunoprophylaxis as an adjunct to chemoprophylaxis • Serogroup B is only weakly immunogenic and protection must be acquired naturally from exposure to cross-reacting antigens
REVIEW of Neisseria
General Characteristics of Neisseria spp. • Aerobic • Gram-negative cocci often arranged in pairs (diplococci) with adjacent sides flattened (like coffe beans) • Oxidase positive • Most catalase positive • Nonmotile • Acid from oxidation of carbohydrates, not from fermentation REVIEW
Neisseria Associated Diseases (ophthalmia neonatorum) REVIEW
General Overview of Neisseria gonorrhoeae • Readily transmitted by sexual contact • Gram-negative diplococci flattened along the adjoining side • Fastidious, capnophilic and susceptible to cool temperatures, drying and fatty acids • Requires complex media pre-warmed to 35-37C • Soluble starch added to neutralize fatty acid toxicity • Grow best in moist atmosphere supplemented with CO2 • Produce acid from glucose, but not from other sugars REVIEW
Epidemiology of Gonorrhea • Seriously underreported sexually-transmitted disease • 350,000 reported cases in 1998 • Found only in humans with strikingly different epidemiological presentations for females and males • Asymptomatic carriage is major reservoir • Transmission primarily by sexual contact • Lack of protective immunity and therefore reinfection, partly due to antigenic diversity of strains • Higher risk of disseminated disease in patients with late complement deficiencies REVIEW
Pathogenesis of Neisseria gonorrhoeae • Fimbriated cells attach to intact mucus membrane epithelium • Capacity to invade intact mucus membranes or skin with abrasions • Adherence to mucosal epithelium • Penetration into and multiplication before passing through mucosal epithelial cells • Establish infection in the sub-epithelial layer • Most common sites of inoculation: • Cervix (cervicitis) or vagina in the female • Urethra (urethritis) or penis in the male REVIEW
Virulence Factors Associated with Neisseria gonorrhoeae REVIEW
See Handout on Sensitivity & Specificity of Diagnostic Tests (Next two slides)