Download
1 / 31
330 likes | 593 Views
Neisseria. 王淑鶯 微生物免疫學所 國立成功大學醫學院 分機 : 5634 Email: sswang23@mail.ncku.edu.tw. Reference: Chapter 29 in Medical Microbiology (Murray, P. R. et al; 6th edition, 2009). Neisseria. German physician A. L. S. Neisser, who originally described the organism response for gonorrhea.

E N D
Neisseria 王淑鶯 微生物免疫學所 國立成功大學醫學院 分機: 5634 Email: sswang23@mail.ncku.edu.tw Reference: Chapter 29 in Medical Microbiology (Murray, P. R. et al; 6th edition, 2009)
Neisseria • German physician A. L. S. Neisser, who originally described the organism response for gonorrhea
Albert Ludwig Sigesmund Neisser was born as the son of a well known Jewish physician, Moritz Neisser. Neisser began his medical studies in Breslau in 1872. Neisser originally planned to become a specialist in internal medicine, but there was no opening for assistants in Biermer's clinic. It was therefore purely by chance that he turned to dermatology and became an assistant physician to in the dermatology clinic originally founded by Heinrich Koebner. He worked here for two years, and it was here, in 1879, Neisser discovered the gonococcus.
Neisser's discovery occurred in the wake of the rapid development of the new field of bacteriology. It was made possible in large part by his close association with Ferdinand Cohn, the botanist who also gave invaluable help to Robert Koch. Cohn taught him Koch's smear tests for the identification of bacteria. He at first called the microorganism that he thus observed "micrococcus"; they were then given the name "gonococcus" by Paul Ehrlich. Although his discovery was extremely important, it was not until the advent of penicillin that this widespread disease could be controlled. His students called him the "father of gonococcus".
Important Human Pathogens Neisseria gonorrhoeae Neisseria meningitidis Other species normally colonize mucosal surfaces of oropharynx and nasopharynx and occasionally anogenital mucosal membranes. These species have limited virulence and generally produce disease only in compromised patients.
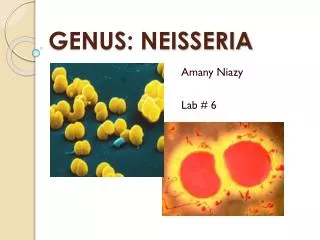
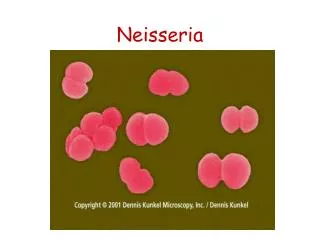
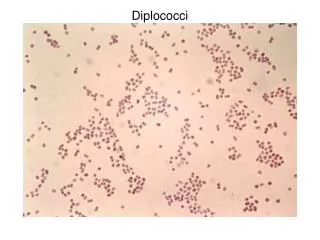
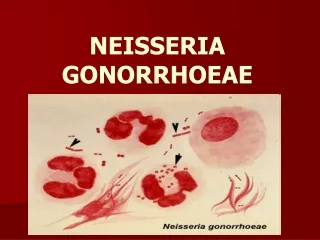
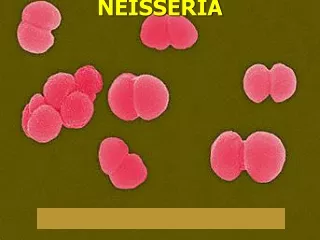
Neisseria N. gonorrhoeae (gonococcus): gonorrhea N. meningitidis: meningitis Morphology and Identification Gram-negative cocci (kidney-shaped), usually in pairs. Human pathogens (i.e. N. gonorrhoeae and N. meningitidis) are typically found associated with or inside PMN cells. They are able to multiply inside the phagocytes, epithelial and endothelial cells. www.buddycom.com
Morphology and Identification Both meningococci and gonococci are encapsulated: menigococci have a polysaccharide capsule; gonococci have a loose capsule-like structure. Grow best under aerobic conditions Produce cytochrome oxidase (oxidase-positive). Meningococci and gonococci grow best in medium containing complex organic substances (e.g. blood, hemin, and animal proteins), and in a humid atmosphere containing 5% CO2. Meningococci and gonococci are rapidly killed by drying, sunlight, moist heat and many disinfectants. Poor survival at cooler temperature.
N. gonorrhoeae (Gonococcus) Antigenic structure 3. Opa: associated with opaque colonies; an outer membrane protein functioning in attachment to host cells. 4. Rmp: stimulates antibodies that block serum bactericidal activity. 5. Lipooligosaccharide (LOS): lacking long-antigenic side chains; endotoxic. 6. Other proteins. 1. Pili: enhancing attachment to host cells and resistance to phagocytosis; antigenically different among strains, and a single strain can make many antigenically distinct forms of pilin. 2. Por proteins: form porins and mediate resistance to neutrophil and serum killing. N. gonorrhoeae is capable of changing its surface antigens (particularly pilin) rapidly to avoid host defenses.
Lipopolysaccharide (LPS) is also called endotoxin. LPS is composed of lipid A, core polysaccharide, and O-specific polysaccharide. Lipid Aanchors LPS in the lipid bilayer. It causes symptoms associated with endotoxin. O-specific polysaccharide can be used to identify certain species and strains. Back
Pathogenesis Attachment to mucosal cells (requires pili) Invade into the cells and multiply (Opa mediates tighter association with and invasion of host cells; Por inhibits phagolysosome fusion) Pass through the cells into the subepithelial space Establish infection (LOS stimulates inflammatory response; Rmp blocks bactericidal activity)
Pathogenesis and Pathology Gonococci attack mucous membrane of the genitourinary tract, eye, rectum, and throat, producing acute suppuration that lead to tissue invasion; this is followed by chronic inflammation and fibrosis.
Epidemiology Gonorrhea occurs only in humans. Gonorrhea is transmitted by sexual contact, often by women and men with asymptomatic infections. Women have a 50% risk of acquiring the infection with a single exposure to an infected man while men have a 20% risk in the same situation. 95% infected men and 50% infected women have acute symptoms. So, asymptomatic carriage is more common in women than in men. Rectal and pharyngeal infections are more commonly asymptomatic than genital infections.
Symptoms 1. Male: urethritis with yellow, creamy pus and painful urination. The process may extend to the epididymis (附睪炎). As suppuration subsides in untreated infection, fibrosis occurs, sometimes leading to urethral strictures (sterility).
2. Female: infection starts from the endocervix (子宮頸內膜) , and results in vagina discharge, dysuria (排尿困難) , and abdominal pain. Uterine tubes may be involved, causing salpingitis (輸卵管炎), fibrosis, and obliteration of the tubes (20% may become infertile). When gonococcal cervicitis is either asymptomatic or unrecognized, the patient may progress to pelvic inflammatory disease (PID).
Gonococcal ophthalmia neonatorum : • bilateral conjunctivitis often follows vaginal delivery from an infected mother. The symptoms are eye pain, redness, and a purulent discharge. The organism can cause permanent injury to the eye in a very short time; prompt recognition and treatment are essential to avoid blindness. prevention: 1% tetracycline, 0.5% erythromycin or 1% silver nitrate eye ointment. (新生兒結合膜炎)
4. Gonococcal bacteremia (1-3% of infected women and much lower percent of infected men) can lead to fever, pustular (膿泡) rash over the extremities, tenosynovitis (腱鞘炎) and suppurative arthritis.
FrequencyIn United States • Incidence is 360,000 infections reported in 2006. • The reported rate is approximately 240 cases per 100,000 population. • The rate of gonorrhea is much higher in African compared to other racial groups. • The rate is associated with socioeconomic and behavioral factors.
FrequencyInternational • Disease rates are unknown for most developing countries. • The incidence is substantially lower in most European countries. • The indigenous gonorrhea has virtually been eliminated in Sweden. • The median prevalence of gonorrhea has been estimated to be 10% in Africa, 5% in Latin America, and 4% in Asia.
Age • In the United States, the highest rates of gonorrhea are found in young (15-24 y) unmarried persons and in groups of low educational and socioeconomic status. • Infection in children is a marker for child sexual abuse.
Immunity Treatments Repeated gonococcal infections are common, because protective immunity to reinfection does not develop due to the antigenic variation of gonococci. This makes development of effective vaccines difficult. Resistance to penicillin G (PPNG: penicillinase-producing N. gonorrhoeae) and tetracycline is common. Resistance to fluoroquinolones has also become prevalent. Ceftriaxone can be used for uncomplicated gonorrhea. In gonococcal infections other than urethritis in men, cure should be established by follow-up, including cultures from the involved sites.
Laboratory Diagnosis Gram stain (gram-negative diplococci in PMNs): Sensitive (>90%) and specific (98%) for men with purulent urethritis. Less sensitive for asymptomatic men (<60%). Relatively insensitive for both symptomatic and asymptomatic women. * Negative results must be confirmed by culture. Culture: Avoid drying of specimen (genital or rectal) and low temperature. Direct inoculation of specimens onto prewarmed media is preferred. Inoculate both the selective media (e.g., modified Thayer-Martin) and non-selective media (e.g., chocolate blood agar; for strains that are sensitive to vancomycin).
Identification N. gonorrhoeae is distinguished from other species by acid production from oxidation of glucose, but not from other sugars. Direct detection of N. gonorrhoeae in clinical specimens by PCR with specific primers.
Prevention and Control Chemoprophylaxis is ineffective except for eye infections. Areas with high incidence of PPNG: Asia, parts of Africa and some places in USA. Infection rate can be reduced by: 1. avoiding multiple sexual partners; 2. early diagnosis and treatment; 3. finding cases and contacts through education and screening of population at high risk. 4. combined with doxycycline or azithromycin for dual infections with Chlamydia
Neisseria meningitidis (meningococcus)
Antigenic structure 1. Capsular polysaccharide: more than 13 serogroups have been identified (serogroups A, B, C, X, Y, and W135 are most commonly isolated). 2. Pili (allow bacterial colonization of nasopharynx). 3. Outer membrane proteins: these are analogues to the Por and Opa proteins of gonococci. 4. Lipooligosaccharide (LOS): responsible for diffuse vascular damage in meningococcal infections.
Pathogenesis, Pathology, and Clinical Finding Meningococci are human pathogen Like gonococci, meningococci are able to invade the epithelial cells. The capsule of meningococci protects the bacteria from phagocytic destruction. Nasopharynx is the portal of entry attach to epithelial cells with the aid of pili (may colonize without producing symptoms) reach the blood stream, producing bacteremia. Upper respiratory tract infection. Fulminant meningococcemia. (腦膜炎球菌血症)
Fulminant meningococcemia High fever and hemmorrhagic rash. There may be disseminated intravascular coagulation (血管內凝集) with shock, and circulatory collapse (Waterhouse-Friderichsen syndrome: bilateral destruction of adrenal gland.) Meningitis is the most common complication of meningococcemia. A milder septicemia with low-grade fever, arthritis, and petechial skin lesions that persist for days or weeks may be observed. Other syndromes: pneumonia, arthritis, and urethritis. Meningococcemia can be prevented by specific bactericidal antibodies in serum.
Meningitis Symptoms: begins suddenly, with intense headache, vomiting, and stiff neck, and progress to coma within a few hours. Mortality: nearly 100% if untreated; <10% in patients treated promptly with appropriate antibiotics. Neurologic sequelae: uncommon; hearing deficit. Skin lesions in a patient with meningococcemia
Immunity Protective immunity is the group- or type-specific, complement-dependent, bactericidal antibodies. Serogroup B, whose capsule contains sialic acid, is relatively non-immunogenic. Treatment Penicillin G is the drug of choice. Laboratory Diagnosis Specimen: blood and cerebrospinal fluid (CSF). >107 bacteria/ml of CSF are normally found in untreated patients. Gram stain: gram-negative diplococci in PMNs. Culture: alternative blood culture methods are required because additives in the blood culture broths can be toxic for this organism. Identification: acid formation with glucose and maltose, but not others.
Epidemiology, Prevention, and Control Meningococcal meningitis occurs in epidemic (in developing countries) and sporadic cases (in developed countries). Transmitted by respiratory droplets among people in close contact (family members; soldiers in military barracks; direct contact with the respiratory secretions of an infected person.) Reduction of personal contacts in a population with a high carrier rate is important for prevention. Rifampin, ceftriaxone, or ciprofloxacin can often eradicate the carrier state and serve as chemoprophylaxis. Persons with deficiencies in the complement system are at high risk for meningococcal disease. Vaccination of specific capsular polysaccharides of groups A, C, Y, and W-135 is used for protecting susceptible persons against infection.Outer membrane vesicle vaccines for group B are being developed recently.
Areas with frequent epidemics of meningococcal disease. This is known as the Meningitis Belt of Africa, and visitors to these locales may benefit from meningitis vaccine. Large-scale outbreaks rates as high as 400-500 cases per 100,000 population (compared to 1-2 cases per 100,000 population in USA).