Download
1 / 5
50 likes | 848 Views
London Patient Choice Project London Patient Choice Project Ophthalmology (Cataract) Care Pathway 31/12/2003 Ophthalmology (Cataract) Patient ( Clinical ) Pathway Principles and Standards Patient Identification Pre - Operative Principles:

E N D
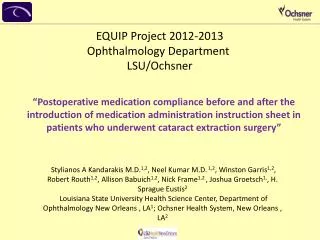
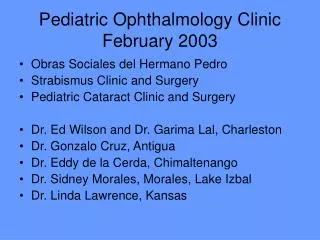
London Patient Choice Project London Patient Choice Project Ophthalmology (Cataract) Care Pathway 31/12/2003
Ophthalmology (Cataract) Patient ( Clinical ) Pathway Principles and Standards Patient Identification Pre - Operative • Principles: • Clear responsibility for ongoing treatment in the best interests of the patient. • Need to work together to provide a high quality experience for patients. • Minimal reasons for excluding patients from being offered Choice - No “cherry picking” by the provider. • Operative Assessment Visit: • Personnel required: Surgeon (with level of experience which would enable performing the surgery) and Nurse • Tests:Biometry, urinalysis, B/P, Bloods (FBC). • Consent • Assessment of suitability for day surgery. • All patients who have been on the waiting list for the agreed procedures for 4 months and 2 weeks and are registered with a London GP (PCT) are eligible to be offered Choice EXCEPT patients in the following groups: • Patients with unstable glaucoma or sight threatening diabetic retinopathy BUT they should also not be amongst those waiting 4 and a half months. • (Now working towards a 3 month maximum wait for cataract surgery) BestPractice Guidelines/Standards Royal College of Ophthalmologists Guidelines - Cataract Surgery 2001 Anaesthesia 2001 Commissioning Cataract Surgery - June 2002 Clinical Governance in ophthalmology - April 1999 Action on Cataracts, DOH - 2000 • There are a number of possible outcomes from this visit - local arrangements to accommodate & track these outcomes MUST be in place. • Patient fit for surgery, wishes to proceed (at RT) & date of operation agreed with patient. • Patient fit for surgery or temporarily unfit for surgery but wishes to have surgery/further treatment at OT. • Patient decides not to proceed with surgery. • Patient is temporarily unfit for surgery - will require treatment at OT or by GP prior to returning to RT for operation. * • Patient not suitable for surgery at any time. * • Surgery is no longer required. • * A clear record must be kept of the clinical reasons which prevent patients progressing to surgery - these outcomes will be audited by the LPCP team. • The RT consultant must also write to the OT consultant with the clinical findings. In the longer term it is recommended that assessment/pre-operative processes are introduced at the initial Outpatients attendance and commenced as soon as the patient is listed for surgery
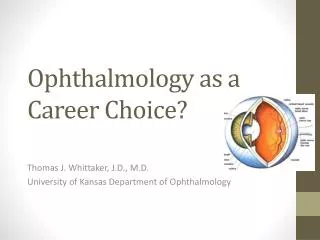
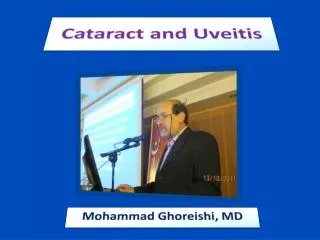
Opthalmology (cataract) patient pathway Planning for Discharge Peri-Operative Post Operative Follow up • The patient should be provided with written information about what to expect on discharge. • They should also be provided with a 24 hour contact number at the RT for any queries arising. (RCOphth June 2002 ~ “The provider units must have adequate arrangements for handling urgent enguiries from patients, it is not acceptable for patients to be told to go to their local A&E) • The RT will provide a minimum of 1 follow up appointment. • Responsibility for the patients (regarding their surgery) remains with the RT until the patient is discharged from this episode. • When cataract surgery is required for the patients 2nd eye, this should be arranged with the patient through the PCA (if the patient so wishes). Ideally this should take place between 1 and 3 months of surgery on the first eye. • RT has responsibility to manage complications appropriately and then refer back to the OT with full information and following discussion with the clinical team at the OT. • The RT has no continuing responsibility if the patient is discharged at the follow up appointment. However, where coninuing care for conditions such as glaucoma or diabetic retinopathy is required, a letter with the appropriate clinical details should be sent the OT. • Surgeon - RCOphth June ‘02 ~ “patients have right to expect that their surgeon has the experience and skill to perform their operation.” In practice this means the surgeon should be a fellow, 3rd year SPR, NCCG of appropriate experience or a consultant. • Workforce • Record keeping as per guidelines • Monitoring of case mix • Action on cataracts guidelines for theatre practice. • Majority of patients should be day cases. • Criteria for safe discharge should be specified. It is not anticipated that complex discharge planning will be required for this group of patients. However, if a patient does present with more complex needs then there must be liaison between RT and OT and a treatment plan agreed.
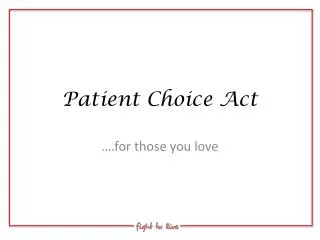
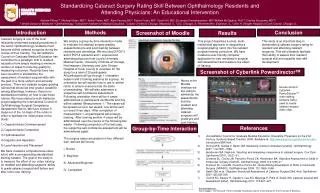
Patient Choice System & PCA Process Principles & Standards Patient Identification Pre Operative Patient Choice System Information about RTs for patients being offered Choice - PCA file RTs will need to provide specific information about Operative Assessment & Operating schedules, ie, Date, Day, Time, Surgeon etc. More slots will be required for Operative Assessment than for operation to allow for patients not proceeding to surgery IT System Development - See separate documents on system development and reporting process (In Guidelines) • Operations should take place within 2 weeks of the pre-operative assessments and can be booked into Choice capacity by the RT. However……. • The outcome of the pre-assessment, including the guaranteed date for surgery and details of any treatment required before surgeryMUST be communicated to the OT, GP and PCA team for reasons of clinical governance, accurate waiting list management and complete patient tracking. If patients receive treatment at OT or by GP in preparation for surgery, RT & PCA team must be made aware of progress via reporting/patient tracking mechanism. • If the date of operation has not already been booked via the PCA the date for surgery MUST be arranged with the patient at the Operative Assessment visit - the patient MUST NOT just be sent an appointment by letter at a later date. • RTs are recommended to use Integrated Care Pathway documentation (which should commence at the pre-operative assessment) to facilitate both accurate & contained record keeping at the RT and comprehensive return of information to the Originating Trust. Rigorous quality assurance process prior to Go Live to ensure operational capacity of participating Trusts - see separate documents. • OT & RTs to establish operational teams with clear roles and responsibilities. • OT will need to log patients excluded from Choice and the reason why against the exclusion criteria - this will be particularly useful as it is anticipated that significant numbers of the patients listed will no longer require the procedure. PCA Process Stage 1: Outpatients Stage 2: Pt. Waiting Stage 3 Choice Offered Stage 4: Choice Accepted Stage 5: Pre-Operative Assessment, Surgery & Discharge
Patient Choice System & PCA Process Planning for Discharge Peri-Operative Post Operative Follow up + Rehabilitation Patient Choice System Patients requiring a second procedure will need to be booked at this stage either by the RT or the PCA. PCA evaluation & feedback. Patient Tracking and reporting process. To ensure a level of equity in Patient Choice, local systems must be known and comply with the timelines of the pathway There are elements of patient care that could be shared between the OT and RT in the best interests of the patient. Copy of RT notes/Integrated Care Pathway to be returned to Originating Trust Outcomes of the completed episode must be reported via Choice template to OT and PCAs. A discharge letter should be sent to the patients GP/Optomotrist in the usual fashion. Patient outcomes should be audited in line with good practice for clinical governance and made available to LPCP clinical advisor for ophthalmology. PCA Process Stage 5 Stage 5 Stage 5 Stage 6: Follow Up