Download
1 / 52
850 likes | 2.34k Views
Lead and Arsenic Toxicity. Lead Poisoning. Physical Properties Lead ( Pb ) has been used by humans for at least 7000 years, because it is widespread, easy to extract, and easy to work with. It is highly malleable and ductile as well as easy to smelt.

E N D
Lead Poisoning Physical Properties • Lead (Pb) has been used by humans for at least 7000 years, because it is widespread, easy to extract, and easy to work with. It is highly malleable and ductile as well as easy to smelt. • Lead’s elemental symbol Pb, is an abbreviation of its Latin name plumbum . • Metallic lead (Pb0) is resistant to corrosion and can combine other metals to form various alloys(Lead alloys are used in batteries, shields from radiation, water pipes, and ammunition) • Inorganic Lead Organic Lead Lead has no known biological function.
Uses and Sources of Lead: • Lead paint: Food containers(painted with lead-based paint or lead-containing glaze , canned foods) • Petrol (tetraethyl lead) • Toys and Jewelry • Herbal remedies from India, China, and other parts of Asia may be potential sources of lead exposure.
Uses and Sources of Lead: • Soil: Exposure to soil that contains particulate lead has been shown to be significantly hazardous for children, who are more commonly exposed by ingestion of house dust or soil than by paint chips. • Water: Drinking water is also a major source of lead Exposure. • Occupational sources: Remodeling construction Smelters Battery factories Ammunition factories • Ceramic glazes . • Soil: Exposure to soil that contains particulate lead has been shown to be significantly hazardous for children, who are more commonly exposed by ingestion of house dust or soil than by paint chips. • Water: Drinking water is also a major source of lead Exposure. • Occupational sources: Remodeling construction Smelters Battery factories Ammunition .
Toxicokinetics • Absorption of Lead: • GI: Children absorb lead well orally (~50%) adults poorly (~10%). Lead absorption is enhanced if diet is poor in iron or calcium. High fat intake and inadequate calories have also been associated with enhanced lead absorption. • Respiratory: Inorganic lead • Skin: Organic lead
Toxicokinetics Distribution: • 95% in bone (%70 in children) • 4% in soft tissue (brain, liver, kidneys, bone marrow) • 1% blood • Lead readily crosses the placenta
Toxicokinetics • Half-life Of Lead • 25 DAYS -- BLOOD • 40 DAYS -- SOFT TISSUE • 20 YEARS -- BONE
Toxicokinetics • Hepatic Metabolism/Excretion • Inorganic lead is not metabolized but is excreted unchanged. • Organic or alkyl-lead,(leaded gasoline, also identified as tetraethyl- and tetramethyl-lead) undergoes oxidative dealkylation to the highly neurotoxin metabolites, triethyl- and trimethyl-lead. • The major route of excretion of absorbed lead is the kidney. Urine: %65 Bile: %35 Children excrete less of their daily uptake than adults, with an average retention in adults of %1-4 versus %33 in children.
Toxic Effects of Lead • Nervous System Neurological, Neurobehavioral, and Developmental Effects in Children • Clinically overt lead encephalopathy may occur in children with high exposure to lead, probably at BLL of 70 μg/dL or higher. • Symptoms of lead encephalopathy: Lethargy Vomiting Irritability Loss of appetite Dizziness Progressing to obvious ataxia, and a reduced level of consciousness, which may progress to coma and death
Toxic Effects of Lead Neurological, Neurobehavioral, and Developmental Effects in Children • The pathological findings at autopsy are severe edema of the brain due to extravasations of fluid from capillaries in the brain. This is accompanied by the loss of neuronal cells and an increase in glial cells. • Recovery is often accompanied by sequelae including epilepsy, mental retardation, and, in some cases, optic neuropathy and blindness. • Most studies report a 2- to 4-point IQ deficit for each μg/dL increase in BLL within the range of 5–35 μg/dL.
Toxic Effects of Lead Neurological, Neurobehavioral, and Developmental Effects in Children • Lead can affect the brain by multiple mechanisms: • Lead may act as a surrogate for calcium and/or disrupt calcium homeostasis. • Lead affects virtually every neurotransmitter system in the brain, including glutamatergic, dopaminergic, and cholinergic systems. (All these systems play a critical role in synaptic plasticity and cellular mechanisms for cognitive function, learning, and memory.)
Toxic Effects of Lead • Neurotoxic Effects in Adults • CNS : Fatigue, irritability, lethargy, insomnia, headache, difficulty concentrating, memory loss and tremor. Sever lead intoxication can result in an encephalopathy characterized by depressed consciousness, seizure, and coma, in association with cerebral edema. • PNS: More than a half-century ago, foot drop and wrist drop characterized the house painter and other workers with excessive occupational exposure to lead. Axonopathy motor disturbance Upper extremities, extensor
Toxic Effects of Lead • Hematologic Effects Lead has multiple hematologic effects,ranging from increased urinary porphyrins, coproporphyrins, δ-aminolevulinic acid (ALA), and zinc-protoporphyrin to anemia.
Toxic Effects of Lead • Renal Toxicity Acute lead nephrotoxicityconsists of proximal tubular dysfunction and can be reversed by treatment with chelating agents. Chronic lead nephrotoxicityconsists of interstitial fibrosis and progressive nephron loss, azotaemia and renal failure. • Fanconlike syndrome • A characteristic microscopic change is the presence of intranuclearinclusion bodies.
Toxic Effects of Lead • Effects on Cardiovascular System The most important manifestation of lead toxicity on the cardiovascular system is hypertension. • The pathogenesis of lead-induced hypertension is multifactorial including: (1) Inactivation of endogenous nitric oxide and cGMP, possibly through lead-induced reactive oxygen species. (2) Changes in the rennin–angiotensin–aldosterone system, and increases in sympathetic activity, important humoral components of hypertension. (3) Alterations in calcium-activated functions of vascular smooth muscle cells including contractility by decreasing Na+/K+-ATPase activity and stimulation of the Na+/Ca++ exchange pump. (4) Possible rise in endothelin and thromboxane.
Toxic Effects of Lead • Reproductive system Impairment of both male and female reproductive function is associated with over plumbism. • Gastrointestinal Lead colic is a major gastrointestinal symptom of severe lead poisoning, and is characterized by abdominal pain, nausea, vomiting, constipation, and cramps. It is rarely seen today.
Toxic Effects of Lead • Bone Effects Lead has an extremely long half-life in bone, accounting for over 90% of the body lead in adults. Lead can affect bone by interfering with metabolic and homeostatic mechanisms including parathyroid hormone, calcitonin, vitamin D, and other hormones that influence calcium metabolism. Lead substitutes for calcium in bone. Lead is known to affect osteoblasts,osteoclasts, and chrondrocytes and has been associated with osteoporosis and delays in fracture repair. In children exposed to lead, a higher bone mineral density (BMD) was observed.
Carcinogenicity • 2B. Agent is possibly carcinogenic to humans • Human epidemiology data weak • Animal data positive
Children Vulnerability • CHILDREN are more vulnerable exposure than ADULTS Size Consume More Food Inhale More Air Developing Nervous System Increased need for Calcium
Recommended Lead level <0.48 (10µg/dl) • < 0.48µmol/l (10µg/dl)=NHMRC Goal. • >0.48µmol/l (10µg/dl)= elevated. • >0.72µmol/l (15µg/dl)=substantially elevated. Notifiable level. • >1.20µmol/l (25µg/dl)= dangerously elevated. >2.20µmol/l (45µg/dl)= Symptomatic
Blood lead concentration (µg/L) Children: <400 Adults: <400 400-500 400-600 500-700 600-1000 >700 >1000 GI Tract Nil ±Abdominal pain ±Constipation Abdominal pain, constipation, weight loss, loss of appetite Abdominal colic, vomiting Blood Subclinical inhibition of RBC enzymes Subclinical inhibition of RBC enzymes Mild anaemia Severe anaemia CNS Effects on IQ in children? Mild fatigue, irritability, slowed motor neurone conduction Fatigue, poor concentration [Peripheral neuropathy] Encephalopathy - delirium - ataxia - fits - coma Other Nil Muscle pain Hypertension, nephrotoxicity, lowered Vit D metabolism Hypertension, nephrotoxicity, lowered Vit D metabolism Clinical Presentation
Managment • IDENTIFY & REMOVE from SOURCE • Nutrition Therapy: Diets high in iron and calcium ● Examples of foods high in iron are: *Cheese, fish, meat, eggs, beans, spinach, raisins ● Examples of foods high in calcium are: * Milk, cheese, ice cream, yogurt, bread, fish, meat, broccoli, fruit, nuts
Chelating Therapy • Consider the use of chelation therapy - Chelatonterapy is wildelyrecomended for asymptomatic children with BLL >450µg/l • Increase lead excretion,reduce blood cocentration,and reverse hemotologic markers of toxcity.
Chelating Therapy • EDTA - Sodium Calcium Edetate 1000-1500 mg/m2/d, IV,IM • IV for severe toxicity, particularly encephalopathy • Well tolerated, <1% nephrotoxicity • BAL-Dimercaprol 450 mg/m2/d IM for severe toxicity only, particularly encephalopathy. • DMSA - 2,3dimercaptosuccinic acid Oral administration Well tolerated . The main problem is foul taste and smell !! Minimal side effects in decade of experience. Displaced D-penicillamine as oral agent since 1991. If adverse reactions to succimer, EDTA, D-penicillamine is the alternative.
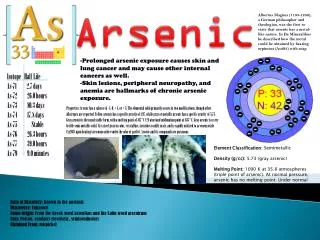
ArsenicIntroduction • Arsenic has been known and used since ancient times as the Poison of Kings and the King of Poisons • Arsenicals have been used since ancient times as drugs and even today are very effective against acute promyelocytic leukemia • Inorganic arsenic exists in the trivalent and pentavalent forms: • Inorganic trivalent arsenic: arsenic trioxideandsodium arsenite, • Inorganicpentavalent arsenic:sodium arsenate, arsenic pentoxide, and arsenic acid • Arsine (AsH3) is an important gaseous arsenical
Arsenic Introduction • Organic Arsenic: • Less toxic that inorganic As • Produced by Biomethylation • Organisms in soil and water • Humans (detoxify inorganic As) • High in shrimp
ArsenicIntroduction • Arsenic is common in the environment • Sources • Groundwater • Arsenic containing mineral ores • Industrial processes • Semiconductor manufacturing (gallium arsenide) • Fossil fuels • Wood treated with arsenic preservatives • Smelting (copper, zinc, lead) and refining of metals and ores • Glass manufacturing
ArsenicIntroduction • Commercial products • Wood preservatives • Pesticides • Herbicides • Fungicides • Food • Seafood and fish • Soil pica behavior: when children ingest large amounts of soil at a time (e.g. up to 1 teaspoon or 5,000mg)
ArsenicToxicokinetics(absorbtion) • Inorganic arsenic is well absorbed (80–90%) from the gastrointestinal tract. • Often metabolized by methylation, and then excreted primarily in urine. • Arsenic compounds of low solubility (e.g.,arsenic trioxide, arsenic selenide, lead arsenide, and gallium arsenide) are absorbed less efficiently after oral exposure. • Skin is a potential route of exposure to arsenic, and systemic toxicity has been reported in persons having dermal contact with solutions of inorganic arsenic. • Airborne arsenic is largely trivalent arsenic oxide.
ArsenicToxicokinetics(excretion) • Excretion of absorbed arsenic is mainly via the urine • Arsenic has a predilection for skin and is excreted by desquamation of skin and in sweat, particularly during periods of profuse sweating • It also concentrates in forming fingernails and hair • T1/2 of inorganic arsenic in the blood is 10 hrs and of organic arsenic is around 30 hours • 2-4 weeks after the exposure ceases, most of the remaining arsenic in the body is found in keratin-rich tissues (nails, hair, skin)
ArsenicToxicokinetics(metabolism) The intermediate metabolites, methylarsonous acid (MMA3+) and dimethylarsinous acid(DMA3+), are generated during this process, and these trivalent methylated arsenicals are now thought to be more toxic than even the inorganic arsenic species
ArsenicToxicokinetics As5+ (Arsenate) As3+ (Arsenite) Methylarsenite (in liver) Dimethylarsenite (readily eliminated – urine)
ArsenicAcute Poisoning • Ingestion of large doses (70–180 mg) of inorganic arsenic can be fatal • Symptoms of acute intoxication include: • Fever • Anorexia • Hepatomegaly • Melanosis • cardiac arrhythmia • in fatal cases, eventual cardiac failure
ArsenicAcute Poisoning • Acute arsenic ingestion can damage: • mucous membranes of the gastrointestinal tract( irritation, vesicle formation, and even sloughing ) • Sensory loss in the peripheral nervous system is the most common neurologic effect, appearing at 1–2 weeks after large doses (a condition that is reversible if exposure is stopped ) • Anemia and leucopenia(granulocytopenia ), (few days following high-dose arsenic )(reversible) • Acute exposure to a single high dose can produce encephalopathy, with signs and symptoms of headache, lethargy, mental confusion, hallucination, seizures, and even coma
ArsenicAcute Poisoning Manifestations of acute arsenic poisoning
ArsenicAcute Poisoning Arsine gas(ASH3), generated by electrolytic or metallic reduction of arsenic in nonferrous metal production. It is a potent hemolytic agent, producing acute symptoms of nausea, vomiting, shortness of breath, and headache accompanying the hemolytic reaction. Exposure to arsine is fatal in up to 25% of the reported human cases.
ArsenicChronic Toxicity Skin • major target organ in chronic inorganic arsenic exposure • Diffuse or spottedhyperpigmentationand, alternatively, hypopigmentation can first appear between 6 months to 3 years with chronic exposure to inorganic arsenic • Skin cancer is common with protracted high-level arsenical exposure Palmar-plantar hyperkeratosis usually follows the initial appearance of arsenic-induced pigmentation changes within a period of years
ArsenicChronic Toxicity Liver • Characteristic of long-term or chronic arsenic exposure, manifests : • jaundice • abdominal pain • Hepatomegaly • progress to cirrhosis and ascites • even to hepatocellularcarcinom
ArsenicChronic Toxicity Peripheral neurophathy • Repeated exposure to low levels of inorganic arsenic can produce • This neuropathy usually begins with : • sensory changes • numbness in the hands and feet painful “pins and needles” sensation • motor nerves be affected • muscle tenderness • weaknes progressing from proximal to distal muscle groupss • Effects are dose-related
ArsenicChronic Toxicity cardiovascular disease • Peripheral vascular disease has been observed in persons with chronic exposure to inorganic • It is manifested : • acrocyanosis • Raynaud’s phenomenon • progress to endarteritis and gangrene of the lower extremities (Blackfoot disease).
ArsenicCarcinogenicity • The carcinogenic potential of arsenic was recognized over 110 years ago • IARC has classified arsenic as a known human carcinogen, associated with tumors of the skin, lung, and urinary bladder, and possiblykidney, liver, and prostate • It has been difficult to confirm the carcinogenicity of inorganic arsenic in experimental animals
Pathophysiology • Trivalent forms: • bind to sulfhydryl groups leading to inhibition of enzymatic systems • inhibit the Krebs cycle and oxidative phosporylation. These lead to inhibition of ATP production. • Pentavalent forms • can replace the stable phosphate ester bond in ATP and produce an arsenic ester stable bond which is not a high energy bond. • Endothelial damage, loss of capillary integrity, capillary leakage, volume loss, shock • Arsine gas • formed by the reaction of hydrogen with arsenic, and is a potent hemolytic agent
Treatment of acute poisoning • Gastric lavage • Activated charcoal does not bind well inorganic arsenic • Whole bowel irrigation with polyethylene glycol • Skin decontamination in dermal exposure