Download
1 / 10
100 likes | 104 Views
Histamine related Angioedema is similar to the spectrum of full blown anaphylaxis. The treatment of histamine mediated angioedema is much similar to anaphylaxis. More info at https://www.360criticalcare.com/

E N D
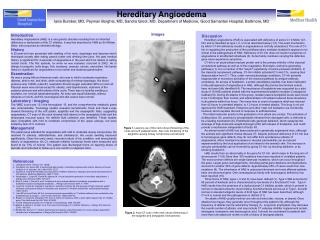
Angioedema in ICU Dr Sananta Dash
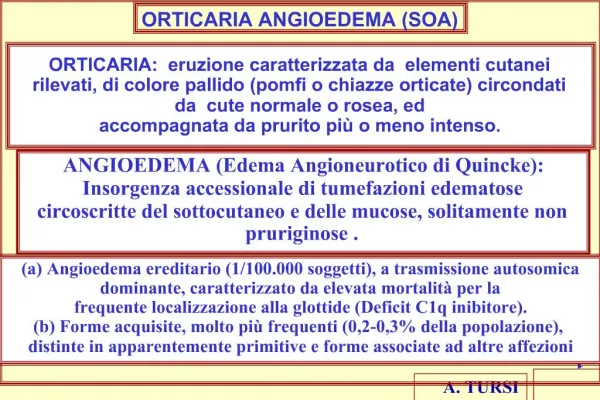
• Angioedema is a medical emergency. • Based on the mechanism, Angioedema may be classified as - Histamine related Angioedema Bradykinin related angioedema
• Histamine related Angioedema Similar to the spectrum of full-blown anaphylaxis Treatment is much similar to anaphylaxis • Bradykinin related angioedoema Differs from the above by its mechanism and the appropriate treatment There are various types of Bradykinin mediated Angioedema
Classification and abnormalities.. Disease Acquired Angioedema Hereditary Angioedema-1 Low C1-INH Hereditary Angioedema-2 Defective C1-INH Hereditary Angioedema with normal C1-INH Factor XII defective Pathology Type 1: Associated Lymphoproliferative disorders (CLL, NHL, Waldestrom’s macroglobinemia etc) Type 2: Associated autoantibody against C1- INH Low Low C4 level Low Low Low Normal Normal Normal C1-INH antigen Low Low Normal Low C1-INH Function C1q Normal Normal Normal Low
History & Clinical presentation: Histamine related Angioedema/Allergic Angioedema Bradykinin mediated Angioedema/Non- allergic angioedema Trigger? Allergens- Food, bites, medications etc Drugs- ACEi, ARBs Minor trauma etc Distribution Symmetric, all-over the body Tongue+ Larynx= 36% Localized, asymmetric Tongue+ Larynx= 59% Prior personal history and positive family history may point strongly towards Hereditary Angioedema Medications history i.e ACE-I inhibitor may suggest alternative diagnosis. Onset Rapid Slow Associated skin manifestations Rash, pruritus, flushing No pruritus. Hereditary angioedema- Erythema marginatum Other organs Hypotension Wheeze Nausea, vomiting, diarrhoea May cause diarrhoea, vomiting but usually non-systemic Response to drugs Adrenaline, Steroid Non-responsive to antihistamine, steroids, adrenaline
Infection (e.g. deep neck space infection) Differential Diagnosis & Lab values Functional or factitious stridor Foreign body Superior vena cava syndrome Macroglossia (e.g. due to acromegaly, amyloid, or hypothyroidism) • Lab values sent: Complement level C1-Inhibitor (C1-INH) level
Management:- Indication for intubation - Stridor, dyspnoea, muffled or hoarse voice. - Drooling and inability to handle secretions. - Progressive deterioration of oedema to cause any of the above - Nasolaryngoscopy shows significant laryngeal oedema or impending closure of the posterior pharynx Role of Nasolaryngoscopy: - Delineate whether there is significant laryngeal edema. - Rule out other causes of airway obstruction or edema
Pathophysiology and site of action of drugs Tranexemic Acid Ecallantide- Kallkrein inhibitor • Pathophysiology and site of action of drugs Icatibant- Bradykinin Antagonist
Mechanism of action Tranexamic acid: - Inhibits the conversion of plasminogen into plasmin (critical step involved in amplification of kallikrein activation) - Effective in of bradykinin-mediated angioedema C1-inhibitor concentrate: - Inhibits XIIa and kallikrein (two most important enzymes involved in bradykinin generation) Fresh Frozen Plasma: • FFP replaces: Angiotensin converting enzyme (ACE) [ACEi-induced angioedema] C1-inhibitor [hereditary angioedema has deficient C1-inhibitor activity] Bradykinin Antagonist (Icatibant) and Kallkrein inhibitor (Ecallantide) - No robust evidence for use of the above - Not widely available and very expensive (they are often even harder to obtain than C1-esterase inhibitor concentrate) - For Subcutaneous administration which may not be useful in an acute setting - Icatibant- Found to be ineffective in ACE inhibitor induced angioedema - Ecallantide also was not found to be very effective and caries a 3% risk on anaphylaxis.
Intubation Extubation • Consideration: - • Severity of swelling to start with • External features- visible swelling, tongue swelling • Videolaryngoscopic view vs nasal endoscopy prior to attempt for extubation • Cuff leak test • Extubation in operating theatre Vs in ICU • Extubation over an exchange catheter A Airw irwa ay y m ma an na ag ge em me en nt t Anticipate difficult airway. • The swelling may get worse with airway manipulation. • If there is laryngeal edma, laryngeal mask airway may become ineffective. • May need surgical airway in the first go as orotracheal intubation may be impossible • Procedure: • Awake fibreoptic intubation Vs Awake cricothyroidectomy • Non-respiratory depressant agents for induction: Ketamine, Dexmedetomidine • Preoxygenation • Backup for front of neck approach • Experienced operator • Surgical expertise- (ENT) as back up