Download
1 / 32
620 likes | 2.36k Views
Cardiogenic Shock. Nitasha Sarswat , MD Cardiology Fellow. Types of Shock. Distributive/Septic Shock: variable cardiac output, decreased SVR Hypovolemic Shock: decreased effective circulating volume

E N D
Cardiogenic Shock NitashaSarswat, MDCardiology Fellow
Types of Shock Distributive/Septic Shock: variable cardiac output, decreased SVR Hypovolemic Shock: decreased effective circulating volume Obstructive Shock: circulatory failure caused by physical obstruction, e.g. cardiac tamponade or pulmonary embolism Cardiogenic Shock: decreased cardiac output, pump failure
Definition of Cardiogenic Shock • Inadequate tissue perfusion resulting from cardiac dysfunction • Clinical definition: decreased CO and tissue hypoxia in the presence of adequate intravascular volume • Hemodynamic definition: Sustained SBP<90 mm Hg, CI <2.2 L/min/m2, PCWP > 15 mm Hg • Subset of severe LV failure patients who have non-hypotensivecardiogenic shock: peripheral hypoperfusion with preserved BP
How to identify Cardiogenic Shock History Physical Exam EKG Chest xray Echocardiogram Swan-Ganz Catheter
History: Who gets Cardiogenic Shock? • Acute MI • Pump failure • Mechanical complications: VSD, Papillary septal rupture, free wall rupture and cardiac tamponade • Right ventricular infarction • Other conditions • End-stage cardiomyopathy • Myocarditis • Myocardial contusion • Prolonged cardiopulmonary bypass • Septic shock with myocardial depression • Valvular disease: AS, AR, MS, MR
Evidence of low perfusion • Narrow pulse pressure • Altered mental status • Low serum sodium • Cool extremities • Hypotension with ACE inhibitor • Renal insufficiency Physical Exam: Hemodynamic Profiles in Heart Failure Congestion at Rest No Yes • Signs of congestion • Orthopnea/PND • JVD • Ascites • Edema • Rales (not always) Warm & Dry 5% Warm & Wet 70% No Low Perfusion at Rest Cold & Dry 5% Cold & Wet 20% Yes Stevenson LW. Eur J Heart Fail. 1999;1:251
Physical Exam • CO Cold extremities, distant pulses, acidosis, SvO2. Try to figure out whether a decrease in CO is due to hypovolemiaor due to pump failure. • Pump Failure Distended neck veins, S3, cold extremities • Preload (CVP) Flat or absent neck veins, tachycardia. • Preload (CVP) jugular vein distention, enlarged veins elsewhere • SVR BP and mental state may be NORMAL. Findings: Cold extremities, distant pulses • SVR Hypotension is likely. Patient may be warm with full pulses if CO is normal or elevated. Other valuable studies: • Spot Echo exam of the heart: addresses tamponade, CHF, ischemia, hypovolemia • O2 saturation from CVP line or PICC line: provides indirect but meaningful estimates of the adequacy of DO2, cardiac function.
EKG If STEMI, degree and severity of EKG should agree with severity of clinical condition If ST elevations in precordial leads -> likely anterior MI -> LV pump failure is likely cause If inferior STEMI -> need marked ST elevations with reciprocal ST depressions on EKG. Check RV leads. If no reciprocal changes or RV infarct, think mechanical problems such as papillary muscle rupture Normal EKG (especially with arrhythmias): think myocarditis
Echocardiogram • Overall and regional systolic function • Mechanical causes of shock • Papillary muscle rupture • Acute VSD • Free wall rupture • Degree of mitral regurgitation • Right ventricular infarction • Other causes of shock (tamponade, PE, valvularstenosis)
Right Heart Catheterization If no right heart catheterization is performed: PE, CXR and TTE must clearly demonstrate systemic hypoperfusion, low CO and elevation of LA pressure/PA pressure /RA pressure If the above is not clear, perform right heart catheterization
Right Heart Catheterization • Exclude volume depletion, RV infarction, mechanical complications • Optimize therapy • CO to guide use of inotropic agents • Filling pressures to guide use of vasopressors and vasodilators • Titration to minimum dosage required to achieve therapeutic goals and minimize increases in oxygen demand and arrhythmogenic potential
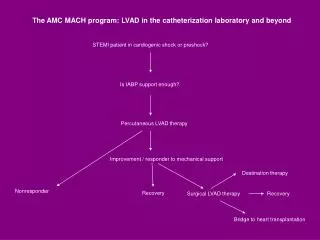
Therapy/Treatment ACC Guidelines Vasopressors and Inotropes Diuretics Cardiac Catheterization Intra-aortic balloon pumps (IABPs) Left Ventricular Assist Devices (LVADs)
Therapy/Treatment: ACC Guidelines Class I 1. Intra-aortic balloon counterpulsation is recommended for STEMI patients when cardiogenic shock is not quickly reversed with pharmacological therapy. The IABP is a stabilizing measure for angiography and prompt revascularization. (Level of Evidence: B) 2. Intra-arterial monitoring is recommended for the management of STEMI patients with cardiogenic shock. (Level of Evidence: C) 3. Early revascularization, either PCI or CABG, is recommended for patients less than 75 years old with ST elevation or LBBB who develop shock within 36 hours of MI and who are suitable for revascularization that can be performed within 18 hours of shock unless further support is futile because of the patient’s wishes or contraindications/unsuitability for further invasive care. (Level of Evidence: A)
Therapy/Treatment: ACC Guidelines 4. Fibrinolytic therapy should be administered to STEMI patients with cardiogenic shock who are unsuitable for further invasive care and do not have contraindications to fibrinolysis. (Level of Evidence: B) 5. Echocardiography should be used to evaluate mechanical complications unless these are assessed by invasive measures. (Level of Evidence: C)
Vasopressors and Inotropes Goal: optimize perfusion while minimizing toxicity Close monitoring of mixed venous saturation Invasive hemodynamic monitoring (arterial line, cardiac output monitoring) to guide therapy Inotropes: shift Frank-starling curve to a higher plateau (increased contractility) Low output syndrome without shock: start with an inotrope such as dobutamine Low output syndrome with shock: start with dopamine or norepinephrine
Vasopressors and Inotropes • Dobutamine: B1 and B2, inotropic but also causes peripheral vasodilation • Good for non-hypotensivecardiogenic shock • Start with 5 ug/kg/min, don’t go higher than 20 ug/kg/min • Dopamine: inotrope and vasopressor in hypotensivecardiogenic shock • Up to 3 ug/kg/min – vasodilation and increase blood flow to tissue beds, but no good evidence for “renal-dose dopamine” • Start at 5 ug/kg/min up to 15 ug/kg/min. Good inotropic and chronotropic effect at doses between 3 and 10 ug/kg/min (B1) • Mild peripheral vasoconstriction beyond 10 ug/kg/min (A1)
Vasopressors and Inotropes • Norepinephrine: primarily vasoconstrictor, mild inotrope • Increases SBP/DBP and pulse pressure • Increases coronary flow • Start 0.01 to 3 ug/kg/min • Good for severe shock with profound hypotension • Epinephrine: B1/2 effects at low doses, A1 effects at higher doses • Increases coronary blood flow (increases time in diastole) • Prolonged exposure -> myocyte damage
Vasopressors and Inotropes • Milrinone: phosphodiesterase inhibitor, decreases rate of intracellcularcAMP degradation -> increases cytosolic calcium • Increases cardiac contractility at expense of increase myocardial oxygen consumption • More vasodilation than dobutamine • Can be combined with dobutamine to increases inotropy • Start bolus 25 ug/kg (if pt is not hypotensive) over 10-20 min then 0.25-0.75 ug/kg/min • May be proarrythmic, questionable in setting of acute MI
Vasopressors and Inotropes • Vasopressin: causes vasoconstriction, glyconeogenesis, platelet aggregation and ACTH release • Neutral or depressant effect on cardiac output • Dose-dependent increase in PVR with resultant increase in reflexive vagal tone • Increases vascular sensitivity to norepinephrine • Good for norepinephrine-resistant shock
Diuretics • Mainstay of therapy to treat pulmonary edema and augment urine output • No good data regarding optimal diuretic protocol or whether diuretics improve outcome in renal failure • Lower doses of lasix are needed to maintain urine output when continuous infusions are used • Start at 5 mg/hr, can increase up to 20 mg/hr
Cardiac Catheterization in Cardiogenic Shock • ACC Guidelines: emergent coronary revascularization is the standard of care for CS due to pump failure (acute MI and shock) • Most often demonstrates multi-vessel disease: • Left main disease 23% • 3-vessel disease 64% • 2-vessel disease 22% • 1-vessel disease 14% • Compensatory hyperkinesis: favorable prognostic factor
Intra-Aortic Balloon Counterpulsation Arterial Pressure Standby Counterpulsation Inflation Deflation Inflation Systole Diastole SMH #619 2008
Intra-Aortic Balloon Counterpulsation Reduces afterload and augments diastolic perfusion pressure Beneficial effects occur without increase in oxygen demand No improvement in blood flow distal to critical coronary stenosis No improvement in survival when used alone May be essential support mechanism to allow for definitive therapy
Left ventricular assist devices • Standard • Percutaneous • Tandem Heart • Complete support • Transseptal puncture • Need good RV function • Impella • Complete support • Easy to insert • Also need good RV function
Left Ventricular Assist Devices (LVADs) Components of the Left Ventricular Assist Device. The inflow cannula is inserted into the apex of the left ventricle, and the outflow cannula is anastomosed to the ascending aorta. Blood returns from the lungs to the left side of the heart and exits through the left ventricular apex and across an inflow valve into the prosthetic pumping chamber. Blood is then actively pumped through an outflow valve into the ascending aorta. The pumping chamber is placed within the abdominal wall or peritoneal cavity. A percutaneous drive line carries the electrical cable and air vent to the battery packs (only the pack on the right side is shown) and electronic controls, which are worn on a shoulder holster and belt, respectively.
Tandem Heart™ • Continuous flow • Removes oxygenated blood from LA via trans-septal catheter placed through femoral vein • Returns blood via femoral artery • Shown to • ↓ LAP and PCWP • ↓ MVO2 • ↑ MAP, CO
Impella • Continuous flow • Inserted into LV through AV • Blood returns to descending aorta • Not yet approved in US
Outcomes in Cardiogenic Shock • In-hospital mortality rate: 50-60% for all age groups • Mechanical complications: even higher rates of mortality • Ventricular septal rupture -> highest mortality (87% in SHOCK Registry) • RV infarction: SHOCK – mortality unexpectedly high, similar to LV failure shock despite younger age, lower rate of anterior MI and higher prevalence of single vessel disease • In hospital survival of diabetic patients in SHOCK was only marginally lower than non-diabetic patients