Introduction
10 likes | 154 Views
Microfracture for chondral defects of the knee Mr S. Kaleel , MRCS; Mr Z.Ahmad , MRCS; Mr S. Daivajna , MRCS; Mr C. Servant, FRCS Department of Orthopaedics, Ipswich Hospital, Ipswich, Suffolk, United Kingdom. Ipswich NHS Trust. Introduction

Introduction
E N D
Presentation Transcript
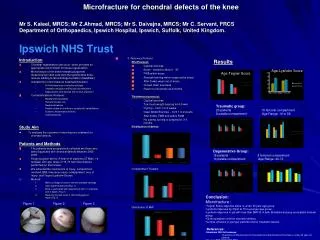
Microfracture for chondral defects of the kneeMr S. Kaleel, MRCS;Mr Z.Ahmad, MRCS; Mr S. Daivajna, MRCS; Mr C. Servant, FRCSDepartment of Orthopaedics, Ipswich Hospital, Ipswich, Suffolk, United Kingdom.Ipswich NHS Trust Introduction • Chondral regeneration can occur when provided an appropriate environment for tissue regeneration. • Microfracture of the bone releases pluripotentmesenchymal stem cells from the subchondral bone marrow leading to fibrocartilage formation (Steadman) • Indications for microfracture treatment(Knutsen) • Full thickness loss of articular cartilage • Unstable cartilage overlying sub-chondral bone • Degenerative joint disease with normal alignment • Contraindications (Knutsen): • Malalignment/Instability • Partial thickness loss • Reciprocal lesions • Patient unable or unwilling to comply with rehabilitation • Systemic Inflammatory Arthritis • Clotting disorder Study Aim ● To evaluate the outcome of microfracture treatment for chondral defects. Patients and Methods • The patients were prospectively collected are those who were diagnosed with chondral defects between 2005-2009 • Single surgeon series: A total of 41 patients (27 Male: 14 females) with age range of 16-73 had microfracture performed on their knees. • We collected the mechanism of injury, compartment involved, BMI, time since injury, compartment, size of injury, and Tegner/Lysholm Scores. • Method: • Make curretage of area to remove unstable cartilage. • Clear subchondral bone(Fig. 1) • Bone is perforated with tapered tool 3mm in diameter and in depth. (Fig. 2) • Resulting clot will result in fibrocartilagenous repair.(Fig. 3) Results • 5. Recovery Protocol: • PFJ Protocol: • Cyclical exercise • Brace - locked to allow 0 - 30° • FWB within brace • Strength training within range set by brace • After 8 wks, wean out of brace • Closed chain exercises • Return to full activity at 4 months • Tibiofemoral protocol: • Cyclical exercise • Toe-touch weight-bearing for 6-8 wks • Cycling – from 1 to 2 weeks • Deep Water Exercise – from 1 to 2 weeks • After 8 wks, FWB and active ROM • No cutting, turning or jumping for 3-4 months • Distribution of defect: • Compartment Treated: • Distribution of BMI: Age-Lysholm Score Age-Tegner Score Traumatic group: 23 patients 15 femoral compartment 8 patella compartment Age Range: 16 to 58 Degenerative Group: 18 patients 8 femoral compartment 10 patella compartment Age Range: 20-73 • Conclusion: • Microfracture : • Tegner Score stays the same in under 40 year age group. • Lysholm improves by 30pts to 73 in younger age group. • Lysholm improves in pts with less than BMI 30 in both tibiofemoral group and patello femoral group. • Gives symptom relief for chondral defects • Is more effective in younger patients and for traumatic lesions • References: • Steadman 2003 Arthroscopy: • Outcomes of Microfracture for Traumatic Chondral Defects of the Knee in under 45 year old patients • Knutsen RCT JBJS 2004,2007 • ACI vs Microfracture 2yr & 5 yr results • Mithoefer: Prospective Cohort; JBJS 2005 • The Microfracture Technique for the Treatment of Articular Cartilage Lesions in the Knee. A prospective cohort study. Figure 1 Figure 2 Figure 3





