Download
1 / 47
470 likes | 645 Views
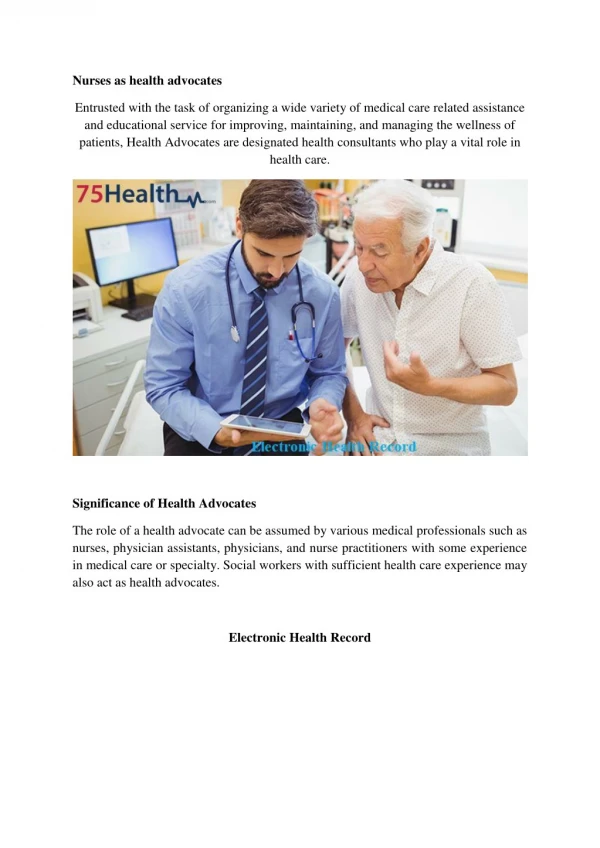
Birth, Death and the Electronic Health Record. Seth Foldy, MD MPH Sethfoldy.com LLC Preventive Health Systems. Big Questions. Will Electronic Health Records (EHR) be an important source of Electronic Birth and/or Death Record Systems data?

E N D
Birth, Death and the Electronic Health Record Seth Foldy, MD MPH Sethfoldy.com LLC Preventive Health Systems
Big Questions • Will Electronic Health Records (EHR) be an important source of Electronic Birth and/or Death Record Systems data? • Should the process of data exchange be partially or completely automated? • When and how should the VR community position itself? • How should the VR community prepare?
Question 1: • Will Electronic Health Records (EHR) be an important source of Electronic Birth and/or Death Record Systems data?
Medicare/Medicaid Electronic Health Records (EHR) Incentive Program(‘Meaningful Use’) • $27B Medicare/Medicaid incentive program (EHR Incentive Program, or ‘Meaningful Use’) is driving EHR adoption • 2009 ARRA HITECH Act • Eligible hospitals and professionals • Financial incentives turn into Medicare penalties after 2016 • National certification requirements for EHRs • Objectives of “meaningful use” of EHR
EHR Use Trending Upward, Pace Quickening Percentage of office-based physicians with EMR/EHR systems: United States, 2001–2010 and preliminary 2011–2012 CDC/NCHS, National Ambulatory Medical Care Survey, 2001–2012.
February – By the Numbers February 2013 – By the Numbers
February – By the Numbers February 2013– By the Numbers
February – By the Numbers February 2013– By the Numbers
February – By the Numbers February 2013– By the Numbers
Who Decides? • Office of the National Coordinator for HIT (HHS, Dr. FarzadMostashari) • Advises HHS Secretary on information standards • HIT Policy and Standards Committees are Federal Advisory Committees (FACA) • Establishes EHR certification requirements • Supports Health Information Exchange (HIE: moving data from one party to another) • Supports privacy and security • Supports research, evaluation, innovation
What does this mean for VR and PH communities? • EHR Systems certified to national standards • Meaningful Use incentives already require some of: • Electronic lab reportable results to public health (hospitals) • Syndromic surveillance • Immunization Information System reporting • Cancer Registry Reporting • Has created pressure on public health systems • Increasing standardized data flow to PH
Beyond the Tipping Point? • 2013 survey (Accenture) 93% of U.S. doctors reported using EHR systems. • More than in France; Singapore; Australia; England; and Canada. • 78% of U.S. physicians routinely enter notes into EHRs; • 65% of U.S. physicians routinely prescribe drugs electronically; • 62% of U.S. physicians receive clinical results in their EHR system, a 24% increase from the prior year; • 57% of U.S. physicians use electronic laboratory orders, a 21% increase from the prior year; • 45% of U.S. physicians use health information exchange technology to access clinical data from outside their organization, a 32% increase from the prior year; and • 38% of U.S. physicians say that using EHRs and HIEs has lowered their organization's costs (Healthcare IT News, 5/9). http://www.ihealthbeat.org/articles/2013/5/10/survey-says-more-than-90-of-us-physicians-now-use-ehrs.aspx#ixzz2UPAfHeO4
Beyond the Tipping Point? • Most health trade groups advocating to continue Meaningful Use incentive program • Many calling for • Slower pace (delay Stage 3) • Fewer requirements (relax Stage 2, or less specificity in Stage 3) • AM News: “Many physicians view electronic health record use like their patients might think of exercise. They don’t necessarily enjoy it while they are doing it, but they recognize and appreciate the benefits.”
NAPHSIS: VR and the EHR • Approximately 99% of all births and 35-40% of deaths in the U.S. occur in hospitals. • Approximately 50% of Birth and Fetal Death data elements are derived from the medical record.
Will Electronic Health Records (EHR) be an important source of Electronic Vital Record Systems (EVRS) data? • YES: EHR replacing paper records • YES: some data reported to VR systems will first be recorded in EHRs as • Structured data (pick-lists, translated, computable) • Unstructured data (text) • Data quality in EHR compared to paper records will: • Increase • Remain same • Worsen • Data will be transferred to VR systems • Manually? • Automatically? • A combination? • The Question: does the VR community desire that • EHRs be certified to standardized collection/reporting of some EVRS data elements? • Providers incentivized to report some data electronically to EVRS?
Issues for VR • Will data be structured in EHR as needed for VR? • Will EHR support additional data entry for VR? • Will EHR data systems support data quality checks for VR? • Will EHR support needed accountability for VR reporters? • Will the process support providers’ and VRs’ business needs?
Question 2: • Should the process of data exchange be partially or completely automated?
Goals for IHE Profile Project • Establish interoperable electronic exchange of VR data between EHR and VR Systems • More timely data release • Higher quality data for demographic and epidemiologic surveillance and research • Less costly electronic vital registration systems • Greater integration with other stakeholder electronic systems • Greater standardization of electronic VR data collection and exchange Michelle Williamson. IHE Quality, Research & Public Health Agenda 8/27/12 http://www.ihe.net/Events/upload/2012-08-24_QRPH_PublicHealth_Focus_IHE_Webinar.pdf
Why Automate Anything? • Improve consistency • Increase speed • Reduce costs Or • Better • Faster • Cheaper
State Registrar/NCHS/PH perspective • BETTER? • Data received more accurate/appropriate/precise? • Data received more complete? • Data elements meet processing requirements? • DEPEND ON ADEQUACY OF EHR CERTIFICATION • FASTER • Delivered to EVRS faster? • Registration accomplished faster? • Transmitted to NCHS faster? • Certificates available to individuals faster? • Statistics and tools (e.g. death index) available for use faster? • DEPEND ON PROVIDER BEHAVIOR, EVRS SYSTEM CAPABILITY • CHEAPER • Less labor per record? • Less labor for follow-ups? • Simplified workflow for record completion? • EVRS cheaper to produce, procure, maintain, replace? • DEPEND ON EVRS SYSTEMS LEVERAGING EHR STANDARDS
Clinical perspective(incl. Funeral Director) • BETTER • Data for quality, safety, & cost management? • Reimbursement or incentives? • Patient satisfaction (effort, access to certificates)? • FASTER • Completion of each registration? • CHEAPER • Less labor per initial record? • Less labor for follow-ups? • Workflow for completion? • EHR cheaper to produce, procure, maintain, replace?
How Important is the Clinical Perspective? • ACA: growing price/performance pressure on hospitals and physicians • If it doesn’t decrease cost, increase income or improve clinical quality, who cares? • Would Registrars or hospitals win a legislative power show-down in your state/territory?
Tentative Conclusion • IF certified EHRs capture well-defined data elements using standardized vocabulary, and • IF EHRs present said data for validation, supplementation, and certification by the health care provider, and • IF this occurs timely in a clinical-friendly workflow, and • IF EVRS systems build toward ONE clear standard for receiving and processing this data, • THEN semi-automated EHR reporting could be better, faster AND cheaper for both clinicians and VR offices
Question 3 • When and how should the VR community position itself? “Need for a long-term, shared strategy for achieving the vision of interoperable vital records systems with electronic health record systems.” Denton Atkinson, NAPHSIS 2012 mtg
In fact, your long term plan is about to intercept Stage 3 Meaningful Use opportunity ? 2012-13 HL7 messages & IHE profile 2009-11 2007 VR Domain Analysis Model 2003 EHR-S VR Functional Profile MoVERS
Is It Time? To achieve consensus on standards… …and advocate they be adopted for Stage 3 Meaningful Use… …and force EHR technology to be certified to the standards… …and prepare to accept electronic transmission?
In your favor: • Slow-down in selection (& maybe deadlines) of Stage 3 Meaningful Use objectives • ONC Standardization and Interoperability Framework activities: • Harmonization of VR data elements with other public health reporting activities in the Public Health Reporting Initiative • Positioned to lead in the Structured Data Capture (SDC) Initiative
Doug Fridsma1: ONC SDC Initiative Initiative’s goal is to identify, evaluate and harmonize four new standards that will enable EHRs to capture and store structured data: • Standard for the structure of the common data elements that will be used to fill the specified forms or templates. • Standard for the structure or design of the form or template (container) that common data elements can sit in. • Standard for how EHRs interact with the form or template. • Standard to auto-populate form or template Focus on research, safety event, and public health reports. May closely adhere to VR work in the Quality, Research and Public Health (QRPH) committee of IHE. 1Director of Standards & Interoperability, ONC
Why Focus on SDC Initiative? • If successful, will likely be given priority in future Meaningful Use stages • If successful process, will be supported by research, safety and public health communities • May be “imposed on” public health community
Three Layers of ExchangeStandards Healthcare Provider Vital Records Secure Transport (PHIN-MS, DIRECT, WebServices) Data Exchange Format (HL7 message, C-CDA document) Content/Vocabulary (LOINC, SNOMED)
Business 2 Business (B2B) Healthcare Provider Vital Records
HIE Organization Model Healthcare Provider Vital Records HIE Organization
Public Health Hub Model Healthcare Provider Vital Records PH Agency Hub
Need to consider possible trade-offs • Balanced scorecard • Data quality • Speed • Convenience, Labor & Cost • Accountability • Pace of Change
What Likely Won’t Work for Meaningful Use (or ANY national standardization) • Forcing data providers/EHRs in different states to use different formats, e.g., • Clinical Document Architecture in one state • HL7 2.5.1 messaging in another • Major differences in reporting requirements between states/territories • Failing to establish some uniform expectations of VRDS vendors
Possible Strategy • Advocate for an acceptable set of SDC standards for birth and/or(?) death records • Seek inclusion in Stage 3 Meaningful Use EHR certification requirements • Consider if VR reporting should be incentivized for hospitals and/or eligible professionals in Stage 3 Meaningful Use • If Stage 3 does not contain VR certification requirements, consider other options for certifying EHRs • Consider certifying EVRS’ to • manage standardized EHR data • acceptable workflows for VR staff
Question 4 • How should the VR community prepare?
Drive Toward Informed Consensus:1. Capability • Establish national strategic/tactical leadership • Trusted federal, state, and territorial leaders • Contributing to national FACAs and other committees • On-going communication with VR programs • Able to make decisions rapidly with appropriate consultation • Designee in each VR program to • Become familiar with core documents: • EHR-S VR Functional Model • VR Domain Analysis Model • VR HL7 message guides and document architecture • IHE profile • Track and comment on SDC Initiative products • Follow pilot test process and evaluations • Educate leadership and staff • Establish connections with PH department Meaningful Use lead, State HIT Coordinator • Support participationin national decision making as needed
Drive Toward Informed Consensus2. Learning • Community examination/discussion of pilot projects • Regular discussion of SDC Initiative process • What are necessary and viable trade-offs in • Data quality • Speed • Convenience, Labor & Cost • Accountability • Pace of Change
Drive Toward Informed Consensus3. Decisions • Birth reporting, death reporting, or both as “first mover” for EHR reporting? • Based on readiness, practicality and desirability • Preferred format (2.5.1, CDA) for receiving EHR information? • In consultation with EHR and EVRS vendors • Are SDC products acceptable and actionable? • May require compromise with other stakeholders (research, safety reporting, other public health programs) • Should SDC VR products be adopted for national use?
Drive Toward Informed Consensus3. Decisions (cont.) • Should SDC or other standards be included in “Meaningful Use” EHR certification in Stage 3 (2016 or 17)? • Should VR reporting be added to Meaningful Use Stage 3 incentive objectives (2016 or 17)? • Will numerous VR programs be ready to receive during Stage 3? • Should VR reporting use a nationally-uniform system of secure transport? • DIRECT? SOAP? PHIN-MS? Other? Or variable?
Drive Toward Informed Consensus4. Advocacy • If green light: advocate for VR standards adoption into Meaningful Use certification • If green light: advocate for VR reporting as a Meaningful Use incentive objective • If green light: advocate for a national standard for secure transport of VR records
Drive Toward Informed Consensus5. Implementation • Initiate discussions with state/territorial PH Meaningful Use leader and State HIT Coordinator regarding: • HIE or Public Health hub management of transport/receiving reports • Ensure EVRS vendors begin adopting national standards • Consider certification • Work with EVRS vendors on workflow redesign for maximum benefit from EHR data • Consider certification • Prepare for on-boarding EHR data providers • Prepare to exploit improved data management capabilities
Conclusion • Opportunity exists—window length? • Assessment and decisions needed • Requires • Capacity (national leadership, local liaisons) • Participation • Learning • Decisions • Trade-offs • Advocacy • Implementation • Payoff depends on EVRS and workflow re-design