Download
1 / 66
660 likes | 1k Views
HYPERTENSION ABC & Update. Mahmoud Khattab, Ph.D. Professor of Pharmacology & Toxicology. Development of Structural and Functional Alterations in the Hypertensive Vessel Wall. Smooth Muscles & Endothelial Morphologic Changes In Hypertension.

E N D
HYPERTENSIONABC & Update Mahmoud Khattab, Ph.D. Professor of Pharmacology & Toxicology
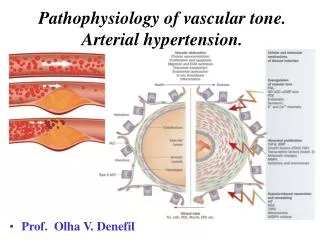
Development of Structural and Functional Alterations in the Hypertensive Vessel Wall
Smooth Muscles & Endothelial Morphologic Changes In Hypertension • The smooth muscle content of arteries can be augmented by an increase in cell number (hyperplasia) or an increase in cell mass (hypertrophy) • The volume of the endothelial cells increases and the surface configuration becomes more globular, so that the cells protrude into the lumen of the vessel
Linkage Between Structural & Functional Changes Poiseuille’s Law: Resistance α 1/r4
Possible mechanisms of Apparent Increased Sensitivity to Vasoconstrictors Patients with essential hypertension have apparent increased sensitivity to forearm infusion of norepinephrine (0.40 μg/min) (increase in resistance) • True increased sensitivity to vasoconstrictors • Increased receptor sensitivity • Increased activation of second messengers or ion channels • Apparent increased sensitivity due to effects of structure or function to increase resistance • Hypertrophy or hyperplasia • Decreased endothelial-dependent vasodilator mechanisms
Characteristics of Hypertension • Elevated BP at maintained cardiac output • Interaction of environmental and genetic factors • Both structural and functional changes in arterioles leading to increased resistance • Structural changes resulting from growth or remodeling of the vessel due to the positive influence of growth factors or the removal of growth inhibitors • Functional abnormalities involving endothelial and vascular smooth muscle dysfunction • Abnormalities in membrane ionic control mechanisms likely underlying abnormalities in both contraction and growth • Enhanced vascular responsiveness to vasoconstrictors
Classification and Goal JAMA 2003;289:2560–2572 • The seventh Report of the Joint National Committee on Detection, Evaluation, and Treatment of High BP (JNC 7)classified hypertension as in the given table • A clinical HTN is based upon two or more seated BP measurements on two more occasions • Ultimate GOALs: • Decrease BP • Reduce associated morbidity manifested as TARGET-ORGAN DAMAGE • CVS risk factors increase frequency of target organ damage (HP+LVH: CHF)
Hypertension -related Target Organ Damage • Brain: stroke/transient ischemic attack • Eyes: retinopathy • Heart: LV hypertrophy, HF, angina • Kidney: chronic kidney disease • Peripheral vasculature: peripheral arterial disease
Heart Promoting atherosclerotic changes (indirectly) Pressure-related: Enhancement of CVD Increase risk for IHD (angina & MI) Antihypertensive therapy reduce such risks Enhance the progress of LVH (LVH+HP; Framingham Study: Increased CHF) BRAIN HTN frequently leads to cerebro-vascular disease as: Transient ischemic attacks Ischemic strokes Cerebral infarcts Antihypertensive therapy reduce the risk of initial and recurrent stroke Hypertension -related Target Organ Damage
Hypertension -related Target Organ Damage Kidney • HP leads to increased intraglomerular pressure causing nephrosclerosis • HTN-Kidney lesion, What comes first? • Chronic kidney disease can proceed to kidney failure (dialysis) • Moderate (Stage 3) Kidney disease (GFR 30-59 mL/min) indicates target organ damage (Creatinine 1.3-1.5 mg/dL) • Albuminurea (>300 mg/day or 200 mg albumin/g creatinine) indicates target organ damage
Peripheral Arterial Disease An atherosclerotic vascular disease equivalent in risk to CAD BP reduction, risk factor modification & antiplatelets are needed to stop progress Complications can attain infection & necrosis EYE Hypertension can induce retinopathy that may proceed to blindness G 1: arterial vasoconstriction G2: Arteriovenous nicking (atherosclerosis) G3: Cotton wool exudates & hemorrhage (untreated HP or accelerated Hypertension -related Target Organ Damage
Major CVS Risk Factors • Age: more than 55 years men, 65 years women • Cigarette smoking • Diabetes mellitus • Hypertension • Dyslipedimia • Obesity • Physical inactivity • Kidney disease: GFR ≤60mL/min
CVS Risk versus BP • Direct correlation between risk of CVD & BP values (epidemiological studies) • Above 115/75 mm Hg, with each increment of 20/10 mm Hg, the risk of CVD doubles • Pre-hypertensive patients are at higher CVD risk than normal • Clinically, elevated SBP is a more predictor of CVD than elevated DBP in patients over 50 years
BP Numerical Values Goal • In most patients, the target BP value is reduce BP lower than 140/90 mm Hg • In diabetic patients and chronic kidney disease patients (estimated GFR ≤60 mL/min or albumin-urea), Coronary Artery Disease (CAD): BP goal is less than 130/80 mm Hg • In LV dysfunction, goal BP is <120/80 • These patients are at high risk for target organ damage
Hypertension Misconceptios • Stress-related: Apart from white coat HP, most HP patients have elevated BP independent of their stress status • Headache (and other symptoms) have no correlation with hypertension • Hypertension though asymptomatic, it has serious long-term complications; long-term therapy • Stress management is not that beneficial in controlling HP • Clinically evidenced, a better quality of life with proper medication; drugs are NOT worsening quality of life
Patient Evaluation/Risk Assessment • Absence or presence of various forms of hypertension-related target organ damage • Identifiable (secondary) causes of hypertension • Concomitant major CV risk factors, other disorders, and assessment of lifestyle habits
HYPERTENSION THERAPYLifestyle Modification • For BP lowering & reduction of CV risk • In prehypertensives: lifestyle modification leads to BP lowering + inhibition or minimizing HTN progress • Possible reduction of dose and/or No of antihypertensive drugs used PATIENT EDUCATION IS NEEDED
Weight Reduction 5-10% wt reduction in overweight persons may lower CV risk For every 1 kg wt loss, there is lowering of SBP & DBP by 2.5 & 1.5 mm Hg respectively DASH Diet Dietary Approaches to Stop Hypertension (DASH) diet is rich in fruits, vegetables & low-at dairy foods, combined to less saturated & total fat A 8-14mm Hg reduction in SBP can be produced Lifestyle Modification
Dietary Sodium Restriction Epidemiology: positive correlation between BP and sodium intake Trials: 2-8 mm Hg reduction in SBP on restricted sodium diet ≤ 2.4 g/day Physical Activity There is 4-9mm Hg reduction in SBP in most patients upon regular PA HTN patients with compromised CVD need medical evaluation before PA Physical activity: at least 30 min for 3-5 days/week Walking, running, cycling, swimming Lifestyle Modification
Smoking Cessation The most important modifiable CV risk factor Cigarette smoking increases CV & total mortality, cessation lowers CVD incidence It interferes with response to some drugs (β blockers) Patient education Unproven Modifications High levels of K+, Ca2+, & Mg2+ relate to lower BP, no reduction of CV risk K+& Mg2+ intake in HP/chronic renal disease may be harmful (cardiac toxicity) Caffeine drinks limitation is not essential unless for other medical reason Lifestyle Modification
Algorithm for Treatment of Hypertension Beta-blockers not first-line in AHA guidelines 2007
Patient Education About Treatment • Assess patient’s understanding and acceptance of the diagnosis of hypertension • Discuss patient’s concerns and clarify misunderstandings • Tell patient BP reading and provide a written copy • Come to agreement with the patient on goal BP • Ask patient to rate (1 to 10) his or her chance of staying on treatment • Inform patient about recommended treatment and provide specific written information about the role of lifestyle, including diet, physical activity, dietary supplements, and alcohol intake; use standard brochures when available • Emphasize: • Need to continue treatment • Control does not mean cure • One cannot tell if BP is elevated by feeling or symptoms; BP must be measured
Evidence-Based Hypertension TherapySELECTION • JNC7 drug therapy algorithm follows evidence-based approach linked to clinical trials interpretation • Thiazide-type diuretic-based therapy leads to significant reductions in: • Stroke (25-47%), Heart attacks (13-27%), All-cause CVD (17-40%), & Survival improvement • Systolic Hypertension in Elderly Program (SHEP), • Swedish Trial of Old Patients with Hypertension (STOP-hypertension) • Medical Research Council (MRC)
Thiazide-Based Therapy versus Newer Agents (The ALLHAT study) • Several clinical trials using newer agents (ACE inhibitors, ARBs, and CCBs) found reduction of BP and CV risk in a similar to thiazides • Possibly ACEIs having better effects • The 2007 AHA HTN guidelines are now the most recent for treatment (Circulation 2007, 115: 2761)
Algorithm for Treatment of Hypertension Beta-blockers NOT 1st line in 2007 AHA guidelines
The ALLHAT Study • The Antihypertensive & Lipid Lowering Treatment to prevent Heart Attack Trial provides recent evidence for thiazide efficacy as used by JNC7 • Designed to testify hypothesis of superiority of newer drugs: amlodipine, doxazosin & lisinopril over the thiazide diuretic chlorthalidone • End-point: combined fatal CHD & non-fatal MI • 42,418 patients for a mean of 4.9 years • Doxazosin arm prematurely terminated because of increased HF risk
The ALLHAT Study • Outcome: No significant difference between chlorthalidone and either amlodipine or lisinopril as regards combined end point • Secondary endpoints pointed to better efficacy of thiazide over amlodipine (less HF) and lisinopril (less combined CVD, HF, & stroke) • Investigators concluded superiority of thiazide diuretics or at least unsurpassed activity • A 2003 network meta-analysis of 42 clinical trials found that low-dose diuretic were most effective first-line treatment for prevention CVD & mortality JAMA;289: 2534 (2003)
Starting Drug Therapy • MONOTHERAPYwhen INITIAL BP IS CLOSE TO GOAL VALUE, 15-20 mm Hg SBP & 10 mm Hg DBP (JNC 7 & others) • STEPPED CARE, • A single drug is chosen & dose increased till BP control occurred, max dose reached, or dose-limiting toxicity • A second drug from a different class is added
Starting Drug Therapy SEQUENTIAL THERAPY • If goal BP is not achieved an alternative drug is chosen, to replace an initial one • It is more advised when the initial drug is not well tolerated or achieved poor BP efficacy Combination Therapy • Encouraged for patients stage 2 hypertension or far from BP goal • Initial combination therapy can be useful for chronic renal disease/diabetes/other resistant patients
THERAPY MONITORING • Four aspects are considered upon monitoring: • BP control evaluated 1-4 weeks after therapy initiation/modification • Initial BP lowering needs 1-2 weeks, but steady BP up to 4 weeks • Average of 2 measurements is used • Standing BP measurement for orthostatic hypotension evaluation (whenever dizziness occurs) • Compliance (adherence) • Progression of the disease; target-organ damage points to therapy modification • Toxicity
Diuretics Thiazides • Are diuretic of choice achieving goal BP values in 50-80% of patients • Hydrochlorthiazide (HCTZ) & chlorthalidone are the most frequently used • Dose of 12.5-25 mg once daily can lower SBP by 15-20 mm Hg & DBP 8-15 mm Hg • Low-dose therapy is equi-effective for both agents according to huge clinical evidence
Diuretics Loop Diuretics • HCTZ is more effective than loop diuretics though less potent • Furosemide is the most frequently used agent, but given more than once daily • They are diuretics of choice in hypertensive patients with severe kidney disease or failure (creatinine 2.5-3 mg/dL) • They are preferred in patients with CHF or severe edema
Diuretics K+-sparing Diuretics • Amiloride/triametrene are reserved for patients developing diuretic-induced hypokalemia • Fixed-dose products including HCTZ & K+-sparing diuretic are available, but initial usage to avoid hypokalemia is not rationalized • They have modest antihypertensive effect when used as monotherapy
Diuretics Aldosterone Receptor Antagonists • Spironolactone & eplerenone cause hyperkalemia, especially in chronic renal disease • Eplerenone is more specific, less gynecomastia but causes greater hyperkalemia • Eplerenone is contraindicated in patients at high risk of hyperkalemia including diabetic 2 patients/albuminurea • Spironolactone is beneficial in hypertensive patients with CHF where it reduces morbidity & mortality • Eplerenone reduces mortality in HF & LV failure in early post MI patients
β-Adrenoceptor Blockers • β-Blockers reduce morbidity & mortality in hypertensive patients with compelling indications; CHF, post-MI, high-risk CHD, & diabetes • All β-Blockers have similar activity on BP lowering • Incidence of side-effects is low in practice and is dose-dependent, i.e., can be minimized with low- to moderate-doses
Pharmacologic Characteristics of β-Blockers NO-Donotaing
Hemodynamic Response to β-Adrenoceptor Blockade • BP decrease after acute response) is modest, with continued treatment the BP decrease becomes much larger in most patients • The magnitude of the decrease in heart rate and cardiac output and the reactive increase in PVR vary with the degree of ISA • These responses do not account for the long-term decrease in BP
β-Blockers • Nonselectiveβ-Blockers are preferred in patients with non-CV indications like migraine prophylaxis/tremor • ISA β-Blockers are indicated for patients responding with severe bradycardia to non-ISA β-blockers • ISA β-Blockers should be avoided in patients with MI history where agonistic properties may worsen the cardiac function
β-BlockersLipid Solubility • Lipid solubility is of max clinical relevance in patients with renal/hepatic impairment • High lipid sol drugs like propranolol are hepatically cleared • Hydrophilic ones (atenolol) have main renal excretion (require dose adjustment) • Lipophilic agents are probably associated with increases CNS side effects like nightmares, depression • High lipid soluble drugs are desirable for migraine prophylaxis due to better CNS access
β-BlockersCompelling Indications • Heart failure (systolic); metoprolol & carvedilol are approved with reduced CV morbidity & mortality • Start with LOW DOSE & gradually increase it • Post-MI & acute MI patients (including relatively contraindicated ones) have prolonged survival & reduced re-infarction • High-Risk CHD: HTN patients with chronic angina or acute CHD (non-ST segment elevation MI & unstable angina) may proceed to fatal MI or others • Decreased HR, contractility & myocardial O2 demand produced by β-blockers reduce the risk
β-BlockersCompelling Indications • Diabetes; a cardio-selective agent is preferred • β-Blockers decrease coronary events, the renal disease progression, and stroke in diabetics • All agents can mask symptoms of epinephrine-associated hypoglycemia (tremors, hunger & palpitations) but not sweating • They cause insulin release inhibition • Non-selective agents can worsen hypoglycemia & prolong recovery from hypoglycemia • β-Blockers are best avoided in Type 1 diabetes but hypoglycemic effects are less common in Type 2 • Non-selective agents should be avoided in “brittle” diabetics especially insulin-dependent patients
ACE InhibitorsEffects of Chronic ACE Inhibition on theRAA System • AngiotensinII disappears from the circulation at peak ACE block • Plasma renin activity, active & inactive renin concentrations increase • The hyperreninemia leads to a rise in plasma angiotensin I levels • The plasma levels of aldosterone are reduced during ACE inhibition • There is an induction of ACE synthesis during long-term treatment
ACE InhibitorsClinical Pharmacological Profile • ACEIs lower BP via peripheral vasodilation with no alteration of CO/HR/or GFR through RAA system &increased vasodilating bradykinin & PGs • Beneficial effects include correction of endothelial dysfunction, LVH regression, insulin sensitivity improvement & collateral vessel development • They can raise serum K+ especially in renal impairment patients • Acute renal compromise in patients with bilateral renal stenosis can occur • Modest creatinine rise, NOT discontinue ACEIs
ACE InhibitorsRisk of Hypotension • First dose ACEIs can induce dizziness, orthostatic hypotension, or even syncope in volume depleted, hyponatremic or exacerbated HF patients • First-dose response is related to increased pretreatment activity of RAA system • Concurrent diuretic therapy may increase the incidence of first-dose response in sensitive patients • Elderly & African American patients mostly have low renin hypertension & less responsive to ACEIs • Diuretic-ACEI combination overcome age- & race-related poor response
ACE InhibitorsCompelling Indications • Heart Failure: ACEI (+diuretic) is considered fist-line & standard regimen in HTN+ systolic HF • Post-MI:ACEI+β-blocker showed reduction of CV risk independent of LV function & BP • High-Risk CHD: ACEIs must be early given in non-ST elevation MI & Unstable angina (as β-blocker) • In chronic angina: ACEI can be added after β-blocker or non-DHP CCB • DiabetesACEIs reduced hypertension-related CV events & nephropathy in diabetic (mostly type 2) patients (HOPE & UKPDS studies)