Download
1 / 58
580 likes | 1.09k Views
The Pregnant Adolescent. And Maternity Nursing in the Community. Rates of adolescent pregnancies, abortions, and live births are significantly higher in the United States than in most other developed countries. Adolescence. The period of transition from childhood to adulthood. Involves change

E N D
The Pregnant Adolescent And Maternity Nursing in the Community
Rates of adolescent pregnancies, abortions, and live births are significantly higher in the United States than in most other developed countries.
Adolescence The period of transition from childhood to adulthood. • Involves change • Often feel a sense of stress and anxiety • Physical changes • Psychological changes
Although specific ages are assigned to.. • Young or Early Adolescents (10 to 13 years) • Middle Adolescents (14-16 years) • Late Adolescents (17-20 years) • Passage of these periods is smooth for some and stormy for others, and some adolescents never complete all aspects of the journey.
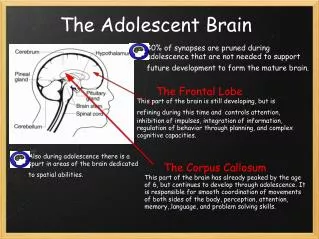
Early Adolescence: 10-13 yrs • Rapid Growth and Development • Physical changes involve all body systems • Menstruation • Breast development • Testicular and penis size • Wet dreams • Exploratory sexual behavior may occur • Rich fantasy life • Peer acceptance & conformity are important • Parental-Adolescent conflict
Middle Adolescent: 14-16 yrs • Physiologic growth & Development of Secondary Sexual characteristics • Appearance (attractive) • Experiment w/ new images • Self-centered • Feel invincible • Risk takers • Drugs • Alcohol • Sex • Unaware of consequences of behavior
Late Adolescence: 17-20 yrs • Ability to maintain stable, reciprocal relationships • Family important but independence is major part of this task • More secure about appearance • Sexual identity is firmly established • Ability to solve problems, assess life situations, delay immediate gratification • Need to think through consequences of not using birth control
ADOLESCENT PREGNANCY Influences on Sexual Behavior
Communication and Visual Images • Communication w/ parents • Open or Limited • Parents send negative messages • Parents live vicariously through teens • Television • Internet • Schools
“Everybody else is doing it – why shouldn’t I” Many adolescent boys and girls become sexually active not because of sexual desire, but because of the need to belong to the group.
Prevention of Adolescent Pregnancy • Sex Education in Schools • Educational Materials • Access to confidential counseling • Access to contraception
Cost of Teen Pregnancy • Taxpayer costs were $9.1 billion in 2004 • Texas costs were $1 billion • Vermont costs were $12 million
Preventing Adolescent Pregnancy • Anticipatory guidance • School education programs • Improved access to health care and counseling • Ready access to nurse or physician • Use of emergency contraceptives, as appropriate • Choice of positive group membership • Choices and ability to use autonomy • Prevention of sexual abuse and date rape
Confidentiality and the Adolescent • Laws vary from state to state • If health care worker cannot provide for confidentiality, some teens will not seek health care • Adolescents are at greater risk for complications of pregnancy, yet are least likely to seek early health care
Medically Emancipated Conditions • Many states do not require parental consent for treatment for • Contraception • Pregnancy • Pregnancy-related care • STIs • Substance abuse • Sexual assault
Date Rape Prevention Teaching Guidelines • Do not get into a vehicle with someone you have just met • When starting to date go on double date, participate in group activities, meet in public places • Provide your own transportation to avoid being alone in a car • Never be alone in a private residence, hotel room or secluded place • Request to drive separately when invited to a party; able to leave if uncomfortable • Do not accept beverages from a stranger • Keep beverages within sight at all times. Dispose of any beverage left unattended • Before dates, tell someone where you are going and when you’ll be home • Plan ahead if your date tried to force or started intimidating you to have sex • Program your cell phone to call 911 with an easy app • Trust your instincts
Incidence of Adolescent Pregnancy • Sociodemographic factors strongly influence birth rate • More than 1 million teenage girls become pregnant each year • Most pregnancies are unplanned • 1 in 17 girls will become pregnant before the age of 20 years • Many have had their first sexual encounter by age 14 years
Health Consequences • Adolescents less likely to receive prenatal care until later in pregnancy • Reasons • Not recognizing pregnancy • Desiring to conceal it • Not understanding value of prenatal care • Not being able to afford or access care
Termination of Education • Pregnancy is the main cause of adolescent girls dropping out of school • Those who have not completed at least high school • Are more likely to be unemployed • Are employed in entry-level jobs • Lack job security
Adolescent Fathers • 1 in 15 boys fathers a child while a teenager • Tend to achieve less formal education • Enter labor force earlier and with less education • Large number of fathers are at least 6 years older than the girl • May be supportive initially, but support may wane over time
Nursing Care of the Pregnant Adolescent Antepartum Postpartum
ANTEPARTUM • Encourage prenatal care • Use Simple Language • Visual Aids • Encourage questions • Good Nutrition • Support • Offer Community services
Labor and Delivery • May not tolerate pain well • Lack of patience • Detailed instructions to support person • Explain everything
POSTPARTUM • Inadequate coping skills • Overwhelmed • Encouragement • Support • Changed self-image • Outcasts • Financial worries • Depression
Adolescent Parenting • May still have unmet needs in own phase of development • Assuming role of parent separates them from their peers • Parenting programs in community • May find they have little social or financial support • Tend to have repeated pregnancies, closely spaced • Can create family instability, further impairing good parenting
UTI’S AND STI’S UTI • Suprapubic pain • Urgency & frequency • Hematuria • Back pain No Vaginal Discharge STI Urinary signs and symptoms WITH Vaginal Discharge
STIs in Adolescents • Unprotected sex has two major consequences in adolescence: unwanted pregnancy and STI • People younger than 25 account for half of new STIs in United States • 1 in 4 adolescents will have contracted an STI by high school graduation • Teens are biologically more susceptible due to epithelium that is present on the cervix and risk-taking behaviors
Reasons Adolescents Do Not Seek Health Care • Limited access • Preference for nonbarrier birth control methods • Involvement with multiple partners • Fear of lack of confidentiality • Lack of knowledge about free programs • Behavioral differences
Teen Pelvic Examination • Key point is to fully inform the adolescent on what to expect • Provide privacy
Treatment Regimens • Single-dose therapy is available for some STIs • Stress importance of completing treatment regimen as instructed to prevent continued infection or the development of a drug- resistant strain
Contraception and Adolescents • Often do not use them correctly • Use or disuse linked to availability, cost, and confidentiality • Some believe using birth control labels them as a “bad girl” • Some teens believe they are protected from pregnancy if the male withdraws before ejaculating
Teaching Adolescents About Contraception • Nurse must consider • Maturity level • Moral and religious beliefs • Motivation to avoid pregnancy • Frequency of intercourse • Regularity of menses • Knowledge of risks of contracting STIs
Elective Abortion • Not an easy decision for most teenagers • Conflicting religious and moral views • May not know where to seek services, learn about other options • Parents may be involved in the decision as to whether to carry the pregnancy to term
Prenatal Programs Available to Adolescents • Three types of programs • Clinic • Private medical services • School-based programs • Choice depends on accessibility and financial circumstances
Community Responsibility • National Campaign to Prevent Teen Pregnancy began in 1996 • Involves adolescents in planning programs • Provides role models from same cultural and racial background • Long-term and intensive programs • Focuses on adolescent needs • Provides nonjudgmental counselors who understand the developing adolescent
PID Pelvic Inflammatory Disease Infection of upper genital tract, Endometrium, Fallopian tubes and adjacent structures • Common complication of STI’s Increased Risk for… • Ectopic Pregnancy • Infertility • Chronic Pelvic Pain later in life
Principles of Effective Interviews and Teaching • Establish Rapport • Assure patients of confidentiality • Full inform • Provide privacy • Be nonjudgmental • Respect maturity of adolescent • Provide open communication lines • Use open-ended questions • Give opportunity for teens to express concerns • Recognize positive success and achievements • Allow sufficient time for interview • Use native language of teen or use an interpreter • Provide follow-up or referral as needed • Provide contraceptive, drug and alcohol information • Discuss high risk behavior • Let the adolescent make final choices and decisions
Risks of Adolescent Pregnancy
Risks • A delay in revealing the pregnancy may limit the options available to the adolescent • The longer an adolescent waits to make decisions on her pregnancy, the higher the risk of negative outcomes (e.g., too late to have elective abortion, failure to obtain appropriate prenatal care early in the pregnancy)
Overview of Issues on OB Home Care: • If they meet certain criteria, both low- and high-risk pregnant women and newborns can be monitored or treated at home • Essential teaching and competencies • Include written instructions • Documentation is used as basis of reimbursement for care provided in home setting
Home Care Settings • Health promotion and disease prevention • Fill gap made by hospital stay, coordinate multidisciplinary care, and make referrals • Can take place in home, short- or long-term care, foster care, and hospice care • Information can be obtained by phone, Internet, electronic monitoring
Protocols and Tools • Emphasis placed on identifying learning needs and skills essential in peripartum • Written materials, help or advice phone lines, Internet • Nurse assists in teaching, caregiving, and preparing woman and family for discharge
Legal Issues • Two types of legal liability • Negligence • Violation of state licensing laws • Reduce risk of legal liability by • Informed consent and clear documentation • Interventions with sound scientific basis and backed by evidence-based practice
Alternative Health Care Practices • Nurse is able to observe cultural practices and alternative treatments being used in the home setting • It is important for the nurse to clearly document what is being used or done in the medical record and also to state what forms of information, education, or training were provided to the patient or caregiver
Home Pregnancy Tests • Now commonly sold over-the-counter in most stores • Considered reliable if performed correctly • If positive, woman should arrange prenatal care as soon as possible • The urine pregnancy test only confirms the presence of human chorionic gonadotropin (hCG); it does not confirm a uterine pregnancy
Prenatal Home Care • Teaching includes • Physiologic and psychological changes • Compliance with prenatal visits • Use of monitors or other special instructions • Common discomforts of pregnancy • Including body mechanics • Home safety and medications
Prenatal Care for Low-Risk Pregnancies • For women with difficulty accessing health care • Transportation, family responsibilities, job • The nurse • Takes a health history • Performs screenings typically conducted in clinic • Fetal heart rate, vital signs, urine screen, weight, fundal height • Provides teaching • Documents all assessments
Prenatal Care for High-Risk Pregnancies • Set standards and criteria must be met for woman to qualify for this type of prenatal care and monitoring • Home care allows for more normal environment, while minimizing family disruption • Nurse discusses importance of rest and determines if any barriers exists • Nurse reviews teachings such as signs of preterm labor, how to place monitoring devices, and need for communication
Postpartum Home Care for Low-Risk Mothers • Sometimes depends on needs of family • Mother is assessed to determine level of recovery and if any complications have arisen • Newborn assessment is also performed • Documentation should include findings, interventions, teaching provided