Download
1 / 25
270 likes | 629 Views
Aging of Cardiac Muscle and Cardiac Failure . Dr. Franco Navazio. Aging Heart in the Elderly. In absence of specific disease the heart adjusts very well to advancing age. Myocardium : Cardiac muscle syncytium (multi-nucleated) Endocardium : Internal layer of heart

E N D
Aging of Cardiac Muscle and Cardiac Failure Dr. Franco Navazio
Aging Heart in the Elderly In absence of specific disease the heart adjusts very well to advancing age.
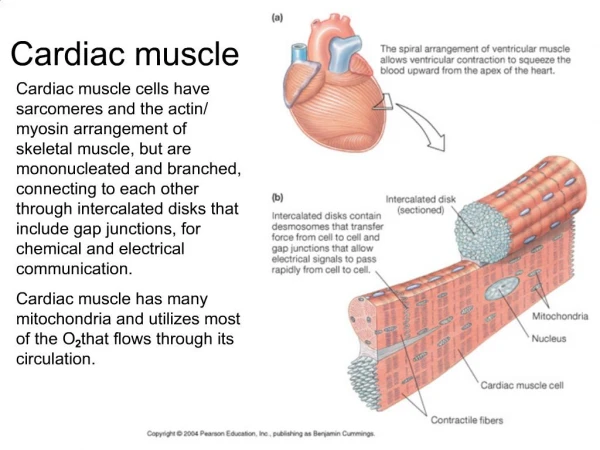
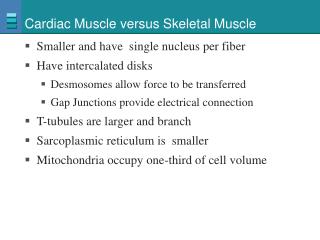
Myocardium: Cardiac muscle syncytium (multi-nucleated) Endocardium: Internal layer of heart Pericardium: External connective tissue layer of heart Valves: openings between cardiac chambers (atrial ventricular) or between heart the arteries (aorta and pulmonary) Conduction system: sinoatrial node (SA) is the pacemaker; also atrial ventricular node (AV), Bundle of His, Purkinje system
Aging Heart: Physiology Decline in the VO2 Max with advancing age Minor decline in the cardiac output Important Variables: • physical conditions • dietary habits Conclusions: Physically fit elderly people have a cardiac physiology similar to younger individuals
Cardiovascular Changes with Age Hypertension: most common treatable cardiovascular change in the elderly Definition: values above 140/190 In young, if standing BP but in elderly it may to 20 mmHg Systolic mumur: 50% of elderly but of very short duration EXG (or ECG): only nonspecific changes due to aging in voltage and nonspecific RBBB Hypotension: diminished baro-reflex response in the elderly. With age, cerebral blood flow but autoregulation acts in a compensatory fashion; some patients maybe affected by symptomatic orthostatic hypotension Orthostatic hypotension: drop of 20 mmHg in the systolic and 10 or more in the diastolic BP on standing upright *MEMO as well as the post-prandial hypotension
Pathology of the Aging Heart Changes due to: • Normal Aging Processes • Superimposed Processes (i.e. endocarditis) • Residuals of other conditions (i.e. hypertension, bicuspid, aortic valve
Aging Heart • Size: can atrophy, remain unchanged or develop moderate hypertrophy. The normal aging heart demonstrates a modest in L ventricular wall thickness. Possible enlargement of the L atrium and L ventricular cavity. • Cardiac myocytes: in size, not numbers (some replaced with fibrous tissue). Cardiac myocytes effective in reentering the cell cycle & proliferating, partly offsetting cell loss due to necrosis or apoptosis. • Amyloid deposition: half of those +70 years have some amyloid deposits in the heart but mostly in small amount & confined to the atria. Amyloid is not present in all elderly persons, not even in centenarians.
Aging Heart • Vasculature (atherosclerosis) • Walls of large arteries thicken, vessels become dilated and elongated • Increase intimal thickness (due to cellular and matrix deposition) • Fragmentation of the internal elastic membrane • Cardiac output (L x min) • not decreased in healthy older men • slightly decreased in older women
Age Associated Changes in Cardiac Function • Overall in systolic BP due to arterial stiffening & in plus wave velocity. Reflects resetting of the baro-receptor reflex to a higher level in the elderly • Myocardial contractility: relaxation is prolonged in senescent cardiac muscle due the sarcoplasmic reticulum seugesters less Ca+2 • Ejection Fraction (EF): no change in resting EF • Heart Rate (HR): supine HR does not change, in sitting and standing positions from 10 to 25%.
Aerobic Capacity & Cardiovascular Function During Exercise in the Elderly With age, peak exercise capacity & peak oxygen consumption slightly but inter-individual variation is substantial Aerobic capacity 50% between 20 years to 80 years: Maximal Cardiac Output (CO) 25% Peripheral O2 utilization 25% (due to in muscle mass & strength) Although the stroke volume in older persons is maintained, age apparently blunts the Frank-Starling mechanism
Heart Failure:Cardiac Output (CO) insufficient to meet physiologic demands In the elderly, heart failure due to: • Mostly systemic arterial hypertension • Coronary artery & valvular diseases (due to impaired cardiac filling & chronic volume overload) • Combined right & left cardiac failure most common, but isolated occurrence of left or right also probable
Heart Failure in the Elderly • Symptoms: dyspnea, orthopnea, fatigue on exertion and dependent edema • Severity: classified according to the NY Heart Association Scale
The Cardiomyopathies:Myocardial disorders without a known underlying cause BUT where other heart diseases may coexistDilated CardiomyopathyHyperthrophic CardiomyopathyRestrictive Cardiomyopathy
Dilated Cardiomyopathy Normal Heart
Hypertrophic Cardiomyopathy Normal Heart
Restrictive Cardiomyopathy: The classic example is the senile cardiac amyloidosis of the elderly, especially over 95 years old. Normal Heart
Cardiomyopathy: Any heart muscle disorder not caused by coronary artery disease, hypertension or congenital valvular or pericardial diseases. Prevalence of heart failure: 25-54 yrs: 1% 55-65 yrs: 3% 65-74 yrs: 4.5% +75 yrs: 10% • > 75% of patients with heart failure +60 years of age • Primary reason is Coronary Heart Disease (CHD) • Secondary reason is Hypertension • Third reason is cardiomyopathy
Sudden Death • In young athletes (also in middle aged men), SUDDEN DEATH can occur in patients with congenital hypertrophic cardiomyopathy • Usually due to severe arrythmia (ventricular fibrillation) • If diagnosis is made a cardiac defibrillator should be implanted. • The SUDDEN DEATH of runners are usually limited to 1 case per 15,000 runners per year-- hence, very rare. • MEMO: There is still the possibility of ANAPHYLACTIC SHOCK in runners or walkers, if stung by a bee.
Syncope in Elderly Definition: temporary suspension of conciousness due to cerebral ischemia Causes • Orthostatic Hypotension • Vaso-Vagal Reflex (?) • Arrhythmias (brady- & tachyarrhythmias) • Drugs • Antihypertensives (vasodilators/diuretics) • Cardiac drugs: beta-blockers, digitalis, anti- arrhythmias, Ca+2 channel blockers, nitrates. • Recreational: alcohol, marijuana and cocaine. • Psychiatric: Antidepressants and phenothiazines
Contributory Causes to Heart Failure in the Elderly • Hypertension (poor elasticity of arterial system) • Alcohol, but only if in excess • Viral infections • Autoimmunity • Heredity (specially for the cardiomyopathies) • Senile amyloid • Diabetes (due to the microvascular disease) • Arrhythmias and especially the TACHYCARDIAS
Conduction System in Aged Heart • Sinoatrial Node: Increased fibrous tissue; seldom origin for arrythmias • Atrio-Ventricular Node: Slight increase in collagen fibers • Bundle of His: Increased fibrous tissue with higher frequency of First or Second degree heart block (the mobitz) • Also the possibility of: L or R BBB (Bundle Branch Block) -this is seldom a complete heart block. • In the conduction system fibrosis occurs: 40% • Coronary Artery Disease : 20% • Calcification : 10%
Normal ECG Ventricular Fibrillation Atrial Fibrillation
Aortic Stenosis:Narrowing of the aortic orifice of the heart or of the aorta itself A common condition due to: • Fatty alteration of collagen • Calcification • Rigidity and various degrees of aortic stenosis • Amyloid infiltration of the valves
Age Specific Lesion: The Valves • Fibrous thickening at sites of closure • Valvular sclerosis caused by collagen and elastic tissue, this is a true wear and tear phenomenon • Calcification of the mitral ring where fatty degeneration invites deposition of calcium • Calcifications is detected in 17 to 45% of patients over 90 years of age • Complications include: heart blocks, infections, embolic