Download
1 / 42
420 likes | 586 Views
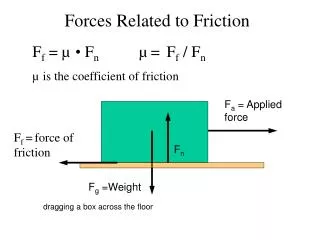
Transdisciplinary Collaboration: A Demonstration Project Phyllis M. Connolly, PhD, RN, CS Jean M. Novak, PhD, CCC-SLP San Jose State University, San Jose, CA. Objectives. Discuss the driving forces related to the need for transdisciplinary collaboration

E N D
Transdisciplinary Collaboration: A Demonstration ProjectPhyllis M. Connolly, PhD, RN, CS Jean M. Novak, PhD, CCC-SLP San Jose State University, San Jose, CA Objectives Discuss the driving forces related to the need for transdisciplinary collaboration Recognize discipline specific assessment tools and interventions use for SJSU Transdisciplinary Project Identify client specific outcomes based on the Omaha Documentation System
Societal Shifts • Nationalism replaced with global economy • Social ecology--needs for integration & connections • Social capital--networks, norms, trust, coordination & cooperation
New organizations New forms of delivery systems-- managed care New ways of relating to each other Smaller companies Outsourcing Disease management High-value organizations depend on and expect workers at all levels to be capable of making decisions Health care being driven by changes in industry TRENDS
Changing Work Environment • Technology • Demographics • Managed Care • Purchaser’s Influence • Health Insurance Industry • Changing Health Systems • Telemedicine
Relationship to Health • Concern not only with costs & benefits but with social, emotional, & physical health • Promoting health and providing health care, no longer the exclusive domain of any discipline • Need for interdependence to improve population health care outcomes
Primary Care: Collaboration Needed Anxiety disorders, depression & substance abuse most frequently misdiagnosed in primary care practices
Project Goal Through collaborative efforts, provide quality, cost effective services for persons with serious mental illness living in the community while simultaneously preparing future mental health professionals for practice.
San Jose State University Office of Sponsored Programs College of Applied Sciences and Arts School of Nursing Nurse Managed Centers Communication Disorders & Sciences: Program & Clinic Department of Occupational Therapy Department of Recreation & Leisure Studies: TR College of Social Work Institute for Teaching & Learning Faculty and Students Revised 5/99 Transdisciplinary Collaboration Project Psychosocial. Occupational Therapy Clinic Santa Clara County Mental Health Santa Clara County Alliance for the Mentally Ill Residents Staff Families ALLIANCE for Community Care Zoe House Crossroads Village Casa Feliz
Definition Collaboration • A dynamic transforming process of creating a power sharing partnership for pervasive application in health care practice, education, research, & organizational settings for the purposeful attention to needs and problems in order to achieve likely successful outcomes (Sullivan, 1998, p. 6)
Transdisciplinary • Refers to a relatively new model based on the concept that the needs of the recipient of services (student, patient, client, etc.) dictates the roles to be performed by members of the team. There can be much overlap in individual job descriptions.
Transdisciplinary Team Advantages • Individualized rehabilitation plan-goals • Integrated service delivery • Role delineation • Reduction of redundant care • Increase of interaction between professionals • Generalization and maintenance of skills • Learning with and from each other • Sharing and growing • Improved quality of life • Cost effectiveness
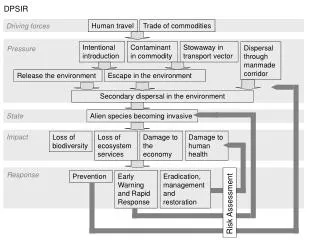
Behavioral Ecological Model of Community Mental Health Laws Administration of Justice University Training of Professionals Community Friends and Peers Church Family Person Laws Mental Health System Social Policy Legislation
Behavioral-ecological Perspective Values & Interventions • Specific values: • Promoting individual competence • Enhancing psychological sense of community • Supporting cultural diversity • Interventions seek to: • Optimize human development • Enhance coping and mastery skills • Enhance organizational and community strengths Improved quality of life
Transdisciplinary Project Caring & Sharing • weekly • campus • case presentation • discipline information • discussion & feedback • 2 days/week • on-site/campus • client contact • experience • implementation • evaluation
Assessment & Outcome Tools • Pragmatic Protocol • Social Skills Rating Scale • Canadian Occupational Performance • Omaha Nursing Documentation System • Allen’s Cognitive Levels • Kohlman Evaluation of Living Skills • Psychosocial Assessment • CERT-Psych
I. Environmental II. Psychosocial III. Physiological IV. Health Related Behaviors I. Health Teaching Guidance, Counseling II. Treatments & Procedures III. Case Management IV. Surveillance Omaha Nursing Documentation SystemDomains Interventions
Communication with community resources Social contact Role change Interpersonal relationship Spiritual distress Grief Emotional stability Human sexuality Caretaking/parenting Neglected child/adult Abused child/adult Growth & development Nutrition Sleep and rest patterns Physical activity Personal hygiene Substance use Family planning Health care supervision Prescribed medication regimen Technical procedure Domain II. Psychosocial IV. Health Related Behaviors
Behavior modification Caretaking/parenting skills Communication Coping skills Exercises Food Interaction Wellness Medication action/side effects Nutrition Rehabilitation Relaxation/breathing techniques Safety Signs/symptoms Stress management Targets
Weight loss Exercise Grooming Safe sex Nutrition Stress management Symptom management Memory Cognition Speech Narrative discourse Conversational skills Social skills Hearing Literacy Issues for Collaboration Health Communication
Primary discipline Assess and evaluate problems and needs Treat & evaluate Seek consultation & referrals Collaborate Supportive discipline Validate treatment approach Assess, treat, recommend Collaborate Approaches to Collaborative Outcomes
Individual One to one Consultation Case Management Health teaching and counseling/guidance Surveillance Treatments & Procedures Referrals Group Psychoeducational classes Modules Activities Health teaching Advocacy Collaborative Interventions
Nursing Assess nutritional status Assess eating behaviors Assess environment Assess and establish exercise program Teach appropriate food selections Evaluate, weigh weekly Communication Disorders Organizing a eating schedule Categorizing appropriate food choices Follow up comprehension Food preparation Weight Loss
Nursing Crisis intervention Deep breathing Self talk Time out Visualization Prevention Diet & nutrition Exercise Time management Communication Disorders Organizing and creating schedules Follow up on comprehension Routines Social skills Stress Management
Communication Disorders interventions Scheduling Visual, writing notes, Reminders Calendars Routines Self generated strategies Repetition Rehearsals Nursing interventions Assess for physiological causes Assess for nutritional status Assess medication efficacy Develop collaborative plan utilizing memory enhancement strategies Memory
Communication Disorders Oral facial evaluation Oral motor exercises Voice Exaggerated enunciation Oral facial awareness Rate of speech Nursing Assess AIMS Assess medication Assess oral hygiene Assess dental hygiene Assess nutritional status Follow up on oral motor exercises Speech (Dysarthria)
Difficulty with Intelligibility Topic maintenance Organizational skills Withdrawal Interventions Outcomes Decrease in rate of speech Increased Intelligibility Narrative discourse, expanded utterances, increase volume Self expression Organizational skills Interaction Social interaction Attention and participation CCF # 9012, Problem 21, Speech, Communication, Spring 97
Knowledge: 2 Behavior: 2 Status: 3 Knowledge: 4 Behavior: 4 Status: 4 CCF # 9012, Problem 21, Speech, Nursing, Spring 97 Final Rating Initial Rating
Knowledge: 3 Behavior: 3 Status: 3 Knowledge: 4 Behavior: 4 Status: 4 CCF #9513, Problem 21, Speech, Fall 98 Initial Rating Final Rating
Knowledge: 2 Behavior: 2 Status: 2 Knowledge: 4 Behavior: 3 Status: 3 CCF # 9073, Problem 30,Digestion-Hydration, Spring 99 Final Rating Initial Rating
Knowledge: 2 Behavior: 2 Status: 3 Knowledge: 4 Behavior: 4 Status: 4 CCF # 9033, Problem 21, Speech, Fall 98 - Spring 99 Final Rating Initial Rating
Knowledge: 1 Behavior: 2 Status: 2 Knowledge: 3 Behavior: 3 Status: 3 CCF #9075, Problem 07, Social Contact, Fall 98 - Spring 99 Initial Rating Final Rating
Knowledge: 2 Behavior: 2 Status: 3 Knowledge: 4 Behavior: 4 Status: 4 CCF #9012, Problem 38, Personal Hygiene, Spring 97 Initial Rating Final Rating
Knowledge: 2 Behavior: 2 Status: 2 Knowledge: 4 Behavior: 3 Status: 3 CCF # 9036, Problem 39, Substance Use, Spring 97 Initial Rating Final Rating
Outcomes Interpersonal Relations:Crossroads S 95 - F 98 N = 15 N = 34 N = 28 N = 20 N = 5 Note: Typical interventions: Health Teaching & Surveillance Typical targets: Communication & Interactions
Decrease in symptoms Community tenure Increased use of community resources Attendance at OT Clinic on campus Increased use of City & University libraries Employment More independent housing Participation in City Recreation Program Enrollment in College and University Volunteer jobs Additional Resident Outcomes
Cost Savings StudyCrossroads Village: 1993-94 • N=25 (9 -12 month) By using Crossroads Village, 25 persons achieved tenure with total savings of $369,471 in the following areas: • Locked facility costs • Emergency psychiatric services costs • Acute in-patient psychiatric services costs • Contract services costs
OutcomesFall 1993 - Spring 1999 22,837 hours direct care 321 undergraduates 59 graduate students 10 faculty
Evaluating Student Learning • Transdisciplinary Seminar • Supervision Groups • Logs • Direct Observation • Process Recordings • Care Plans • One to one
Conflicts in missions Supervision of non-nursing students on site Staffing during non-academic times Maintaining faculty interest Role strain Students dropping clients Inadequate space to meet with students Lack of university support Staff turnover Client hospitalizations Communications Cutbacks in county funding Obtaining permission to provide services from conservators and case managers Conflicts with OT clinic schedule Challenges and Issues
Outcomes of Collaboration Clearly, the closer educators, researchers, consumers, practitioners, and families come together in the service area, the more likely that curricula will be reality based and congruent with clients’ needs. At the same time, the possibility of improving the quality of life increases.