Download
1 / 16
460 likes | 1.95k Views
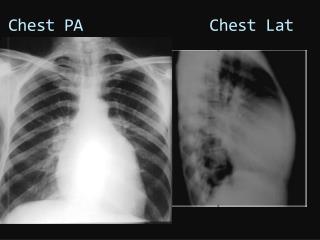
CHEST TUBES. Do’s and Don'ts. Chest Tube Purposes. To remove solids, liquids, and/or gases from the pleural space This allows for lung re-expansion. Chest Tubes. Always keep below chest level NEVER clamp NEVER routinely milk MD should be notified and order obtained.

E N D
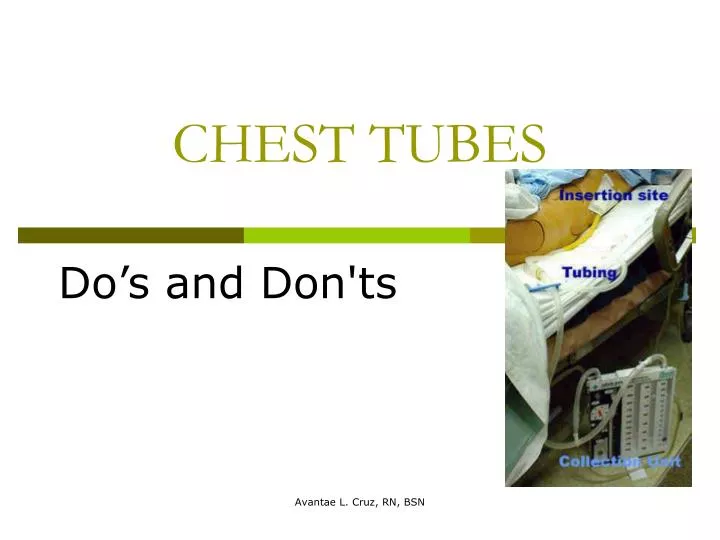
CHEST TUBES Do’s and Don'ts Avantae L. Cruz, RN, BSN
Chest Tube Purposes • To remove solids, liquids, and/or gases from the pleural space • This allows for lung re-expansion Avantae L. Cruz, RN, BSN
Chest Tubes • Always keep below chest level • NEVER clamp • NEVER routinely milk • MD should be notified and order obtained Avantae L. Cruz, RN, BSN
Chest Tube Maintenance • Assess dressing q.48 hours and PRN • Mark hourly shift increments • include date and time • Check and maintain tube patency q.2-4 hrs. • fluctuation of fluid in tubing indicates patency Avantae L. Cruz, RN, BSN
Chest Tube Maintenance • No fluctuation indicates • possible lung expansion • obstructed tubing • improper suction Avantae L. Cruz, RN, BSN
Chest Tube Basics • Assess for air leaks • bubbling in water seal chamber indicates air leaks • Monitor patients pain and treat accordingly • Have patient cough & deep breathe q.2 hr • Vitals q. 2-4 hrs Avantae L. Cruz, RN, BSN
Chest Tube Basics • Observe and report immediately signs of rapid, shallow breathing, cyanosis, complaints of pressure in chest, or symptoms of hemorrhage • ALWAYS keep 2 padded hemostats, sterile water and dressing supplies for possible disconnection Avantae L. Cruz, RN, BSN
Chest Tube Basics • Notify MD for excessive drainage • greater than 100ml/hr • Change in drainage color • Increasing chest pain Avantae L. Cruz, RN, BSN
Chest Tube Basics • If a patient is to be transported place the drainage system below chest level • DO NOT CLAMP THE CHEST TUBE DURING TRANSPORT • clamping cause backflow of fluid into the pleural space Avantae L. Cruz, RN, BSN
Chest Tube Basics • Completely change the drainage system when it nears full • Set-up the new system exactly like the old • Disconnect suction, disconnect the manufacturer’s connection, attach the new system and reconnect suction • THIS IS THE ONLY APPROPIATE TIME TO BRIEFLY CLAMP THE TUBING Avantae L. Cruz, RN, BSN
Chest Tube Basics • If a tube becomes disconnected • clamp at the site of insertion using 2 padded hemostats • Cut off the contaminated tip of the chest tube and tubing; insert a sterile connector into the chest tube and tubing and reattach the drainage system • Cleanse tubing with chloroprep and allow to dry Avantae L. Cruz, RN, BSN
Chest Tube Basics • If the chest tube accidentally slips or is pulled out • IMMEDIATELY cover site with an occlusive dressing; this helps decrease the risk of a pneumothorax Avantae L. Cruz, RN, BSN
Chest Tube Documentation • Patient and family education • Vital signs • Location of chest tube Avantae L. Cruz, RN, BSN
Chest Tube Documentation • Insertion site and dressing • Drainage • Include color and amount • Type of drainage system • water seal vs. suction Avantae L. Cruz, RN, BSN
Chest Tubes • Anytime you have a question please contact the patient’s MD or nursing supervisor Avantae L. Cruz, RN, BSN
Chest Tubes Please refer to POLICY #: NC-A 63.0 Avantae L. Cruz, RN, BSN