Download
1 / 24
240 likes | 441 Views
Interaction between GHI and Health Systems Experience of Uganda. Nelson Musoba Ministry of Health, Uganda. Presentation Outline. Background and Reforms in Uganda’s Health System Examples of interactions between GHIs and Health Systems in Uganda Challenges will be highlighted as we go along.

E N D
Interaction between GHI and Health SystemsExperience of Uganda Nelson Musoba Ministry of Health, Uganda
Presentation Outline • Background and Reforms in Uganda’s Health System • Examples of interactions between GHIs and Health Systems in Uganda • Challenges will be highlighted as we go along
Key Reforms • 1986-1987: Sector Collapsed, Any help was welcome. • 1986-1989: Health Policy Review Commission – consolidation of existing services and re-orientation to PHC • 1995/96 – 2000/01 process of development of the new National Health Policy (NHP) and Health Sector Strategic Plan (HSSP). • Poverty Eradication Action Plan (PEAP) 1997, with updates 2001, 2004; (Poverty Reduction Strategy Papers in other countries) & now • National Development Plan 2009-2013 • All closely aligned to the Millennium Development Goals. • Examples of other reforms; • Decentralisation • National Governance Reforms • Public Service Restructuring
Partnership Principles • Government of Uganda: • To seek donor support only for programs in the agreed framework • To develop comprehensive, costed, prioritized sector-wide programs covering the entire budget, so that government speaks with one voice. • Donors: • To ensure all support is fully integrated into sector-wide programs and is fully consistent with sector priorities • To end individual parallel country programs and stand alone projects • To increase level of delegation to country offices • These Partnership Principles were formulated under the leadership of government (MoFPED, OPM) and in discussion with the highest in country donor & Civil society representation.
SWAp Processes & Structures SWAp structures • Health Policy Advisory Committee – and its technical Working Groups • Joint Review Missions and National Health Assembly • Health Development Partners Group • Tools for SWAp management • National Health Policy and Health Sector Strategic Plan • Memorandum of Understanding • Aide Memoires • Annual Health Sector Performance Report & Mid Term Review Report • SWAp tools and structures are intended to facilitate Joint prioritisation, joint planning, monitoring and evaluation
SWAp • One of the most significant achievements of the SWAp during the period under review was the successful conclusion of negotiations with both GAVI and GFATM towards increased alignment of their support with the health SWAp and agreeing common working arrangements. • Agreement was reached with GFATM on the Long Term Institutional Arrangements (LTIA) for improved alignment of Global Health Initiatives (GHI) support to the sector
SWAp • The GFATM CCM into an expanded Health Policy Advisory Committee (HPAC), • The AIDS CCM into the AIDS Partnership Committee (PC), • Rationalizing the composition of HPAC, and streamlining and revitalizing the Technical Working Groups, including the absorption of the various technical programme Inter-agency Coordinating Committees (ICCs) into the respective Technical Working Groups (TWGs).
Interactions I • Built trust and openness between government and development partners and progressively Civil Society • Planning and Budgeting Process – became more transparent and consultative • Medium Term Expenditure Framework – credible presentation of all public resources (GoU & donor) over a 3 year period • Brings together • Government & Development Partners • Central and District Levels • Public and Private partners
Interactions II • Improved the sector supervision, monitoring and evaluation framework: • The strategic plan includes agreed indicators for monitoring health sector performance • Annual Joint Review Mission (involving GoU – central & Local, donor, private, civil society) – replaced very many review missions by donors • An Annual Health Sector Performance Report produced every year for presentation at the JRM, • Provides a bird’s eye view of sector performance; • Includes a District League Table comparing and ranking performance among districts • Modest increase in Health Sector Public Resource Envelope • Most donors have switched to budget support
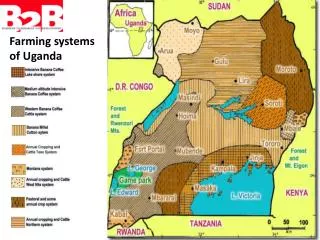
Physical Access • Access to health services is measured by 5 Km walking distance to a health facility (public/PNFP) and is computed from the Health facilities maps, and stood at 72% at the beginning of 2006. Current need is to; • Rehabilitate existing secondary and tertiary health facilities • Strengthen HI management including maintenance • Provide medical equipment There are several sources of funding for the construction of health facilities, many of which it is not possible to have prior information of for planning purposes.
Human Resources for Health • The ever widening gap between the affordable and the optimal HRH requirements. The limited HRH funding for recruitment, salaries and wages, has resulted in recruitment levels being lower than planned; • There is still inequity in the distribution of staff with only 12 of the 80 districts achieving the agreed minimum staffing level of 80%. Related challenges include: Insecurity and remoteness in some parts in the country; and migration of health workers between the sub sectors making recruitment in one result into attrition in another.
HRH II • The time requirements of the HRH management processes – the spread of HRH functions between different stakeholders leads to a lengthy recruitment process including delays in accessing the payroll leading to some prospective applicants withdrawing before taking up the positions; • Low output of some cadres from training institutions e.g Laboratory & Pharmacy Technicians, Medical officers & specialist doctors;
Essential Medicines • Challenges are at the various levels including the national level in terms of medicines procurement and logistics management at the NMS. • inadequate cash flow; • inadequate staffing for medicines management at MoH and local governments; • poor quantification and late ordering by the health facilities and local governments; and • managing the third party items. • The availability of medicines has continued to be a major challenge, at less than 35% in against an annual target of 55% and the HSSP II target of 80%. • There is marked under funding of medicines especially EMHS with less than 30% of requirement for the UNMHCP currently provided for.
How does Infant Mortality in Uganda Compare to other Countries? Deaths per 1,000 live births 2006 UDHS
Trend in Ownership of Mosquito Nets % of households with at least one mosquito net 2006 UDHS
LLIN coverage targets based on availability of nets from GF & partners
Health Sector Budget Allocations by Source FY 2004/05 – 2008/09
LLIN Coverage • Current coverage with LLINs in Uganda is estimated at 40% according (Net mapping report, 2008; Malaria Consortium model, 2007). • LLIN distribution is the mainstay of the country’s prevention strategies. Coverage is expected to drastically increase with Round 7 support which was approved and which will start implementation in 2009/2010. • Under Round 7 a total of 17 million nets will be brought into Uganda and universal coverage is expected by 2011. • However, after 2011, attrition of nets and population growth will reduce coverage with LLINs in the population to approximately 84%, falling to 68% in 2013 and 38% in 2014 (see Figure above). • Need for “keep-up” of nets in 2012 and 2013 in order to maintain coverage at 100%. Mass replacement of nets required for 2014 will be requested in a subsequent round pending distributions of Round 7.
Challenges • Financial - more efficiency (resource allocation & use) - increased investment i.e. new and additional funding • Considerable amounts of resources still managed outside the SWAp • Population growth • High fertility rate • High unmet need for family planning