Download
1 / 1

E N D
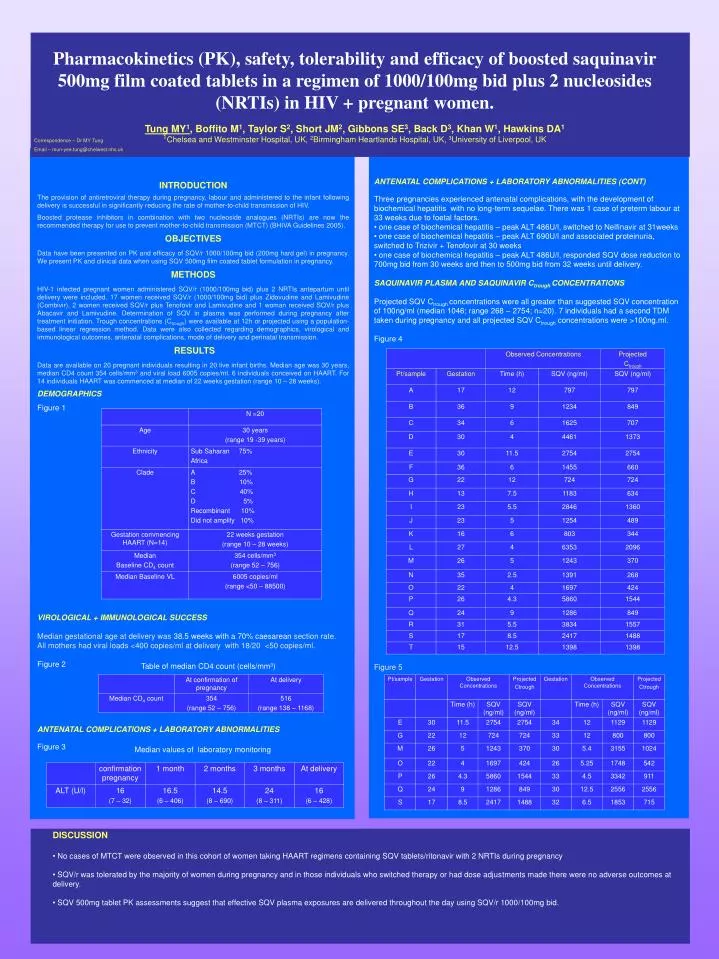
Pharmacokinetics (PK), safety, tolerability and efficacy of boosted saquinavir 500mg film coated tablets in a regimen of 1000/100mg bid plus 2 nucleosides (NRTIs) in HIV + pregnant women.Tung MY1, Boffito M1, Taylor S2, Short JM2, Gibbons SE3, Back D3, Khan W1, Hawkins DA11Chelsea and Westminster Hospital, UK, 2Birmingham Heartlands Hospital, UK, 3University of Liverpool, UK Correspondence – Dr MY Tung Email – mun-yee.tung@chelwest.nhs.uk INTRODUCTION The provision of antiretroviral therapy during pregnancy, labour and administered to the infant following delivery is successful in significantly reducing the rate of mother-to-child transmission of HIV. Boosted protease inhibitors in combination with two nucleoside analogues (NRTIs) are now the recommended therapy for use to prevent mother-to-child transmission (MTCT) (BHIVA Guidelines 2005). OBJECTIVES Data have been presented on PK and efficacy of SQV/r 1000/100mg bid (200mg hard gel) in pregnancy. We present PK and clinical data when using SQV 500mg film coated tablet formulation in pregnancy. METHODS HIV-1 infected pregnant women administered SQV/r (1000/100mg bid) plus 2 NRTIs antepartum until delivery were included. 17 women received SQV/r (1000/100mg bid) plus Zidovudine and Lamivudine (Combivir), 2 women received SQV/r plus Tenofovir and Lamivudine and 1 woman received SQV/r plus Abacavir and Lamivudine. Determination of SQV in plasma was performed during pregnancy after treatment initiation. Trough concentrations (Ctrough) were available at 12h or projected using a population-based linear regression method. Data were also collected regarding demographics, virological and immunological outcomes, antenatal complications, mode of delivery and perinatal transmission. RESULTS Data are available on 20 pregnant individuals resulting in 20 live infant births. Median age was 30 years, median CD4 count 354 cells/mm3 and viral load 6005 copies/ml. 6 individuals conceived on HAART. For 14 individuals HAART was commenced at median of 22 weeks gestation (range 10 – 28 weeks). DEMOGRAPHICS Figure 1 VIROLOGICAL + IMMUNOLOGICAL SUCCESS Median gestational age at delivery was 38.5 weeks with a 70% caesarean section rate. All mothers had viral loads <400 copies/ml at delivery with 18/20 <50 copies/ml. Figure 2 ANTENATAL COMPLICATIONS + LABORATORY ABNORMALITIES Figure 3 • ANTENATAL COMPLICATIONS + LABORATORY ABNORMALITIES (CONT) • Three pregnancies experienced antenatal complications, with the development of biochemical hepatitis with no long-term sequelae. There was 1 case of preterm labour at 33 weeks due to foetal factors. • one case of biochemical hepatitis – peak ALT 486U/l, switched to Nelfinavir at 31weeks • one case of biochemical hepatitis – peak ALT 690U/l and associated proteinuria, switched to Trizivir + Tenofovir at 30 weeks • one case of biochemical hepatitis – peak ALT 486U/l, responded SQV dose reduction to 700mg bid from 30 weeks and then to 500mg bid from 32 weeks until delivery. • SAQUINAVIR PLASMA AND SAQUINAVIR Ctrough CONCENTRATIONS • Projected SQV Ctrough concentrations were all greater than suggested SQV concentration of 100ng/ml (median 1046; range 268 – 2754; n=20). 7 individuals had a second TDM taken during pregnancy and all projected SQV Ctrough concentrations were >100ng.ml. • Figure 4 • Figure 5 Table of median CD4 count (cells/mm³) Median values of laboratory monitoring • DISCUSSION • No cases of MTCT were observed in this cohort of women taking HAART regimens containing SQV tablets/ritonavir with 2 NRTIs during pregnancy • SQV/r was tolerated by the majority of women during pregnancy and in those individuals who switched therapy or had dose adjustments made there were no adverse outcomes at delivery. • SQV 500mg tablet PK assessments suggest that effective SQV plasma exposures are delivered throughout the day using SQV/r 1000/100mg bid.






