Non invasive ventilation and LV dysfunction
Non invasive ventilation and LV dysfunction. Fekri Abroug ICU. CHU F.Bourguiba Monastir. Tunisia. How can cardiogenic pulmonary edema-induced respiratory dysfunction aggravate cardiac dysfunction and circulatory failure ?. Cardiogenic Pulmonary edema. WOB . Exaggerated decrease


Non invasive ventilation and LV dysfunction
E N D
Presentation Transcript
Non invasive ventilation and LV dysfunction Fekri Abroug ICU. CHU F.Bourguiba Monastir. Tunisia
How can cardiogenic pulmonary edema-induced respiratory dysfunction aggravate cardiac dysfunction and circulatory failure ?
Cardiogenic Pulmonary edema WOB Exaggerated decrease in pleural pressure at inspiration Hypoxemia
Cardiogenic Pulmonary edema WOB Hypoxemia risks of myocardial ischemia risks of critical organs hypoperfusion
Cardiogenic Pulmonary edema WOB Exaggerated decrease in pleural pressure at inspiration Hypoxemia Increase in LV afterload
Cardiogenic Pulmonary edema WOB Exaggerated decrease in pleural pressure at inspiration Hypoxemia Increase in LV afterload risks of myocardial ischemia risks of decrease in Stroke Volume
Cardiogenic Pulmonary edema WOB Exaggerated decrease in pleural pressure at inspiration Hypoxemia Increase in LV afterload decrease in CaO2 risks of myocardial ischemia risks of critical organs hypoperfusion risks of decrease in Stroke Volume Risks of aggravation of cardiac dysfunction (vicious circle) and of circulatory failure
How can positive pressure ventilation improve cardiac dysfunction and circulatory failure in patients with cardiogenic pulmonary edema?
Positive pressure ventilation in cardiogenic pulmonary edema WOB Exaggerated decrease in pleural pressure at inspiration Hypoxemia decrease in CaO2 risks of myocardial ischemia risks of critical organs hypoperfusion risks of decrease in Stroke Volume Postive pressure ventilation by breaking the vicious circle prevents aggravation of cardiac dysfunction and of circulatory failure
NIV and Cardiogenic Pulmonary edema (CPE) • NIV: important tool in ARF • Reduces the need for invasive ventilation • Reduces IMV complications • Reduces ICU complications, stay, mortality • CPE common medical emergency • NIV increases cardiac output • Improves gaz exchange • Decreases endotracheal intubation • Trends towards decrease in mortality
Clinical goals in CPE • Improve systemic oxygen saturation • Reduction in LV preload • Reduction in LV afterload • Oxygen through high flow facemask • Morphine • Diuretics • nitrates
CPAP is effective in CPE unresponsive to medical RxPoulton Lancet 1936 • Increase in inspiratory and expiratory flow and pressure • Increases Vt • Unloads inspiratory muscles • Improves alveolar ventilation • Reexpands flooded alveoli • Counteracts intrinsic PEEP • Prevents micro-atelectasis • Improves the P-V curve relation • Increases in intrathoracic pressure reduces the left ventricular preload and afterload • Increases cardiac output in CHF
Both CPAP and bilevel non-invasive ventilation proved effective in treating CPE Better than conventional oxygen therapy
Intubation rate: 5% vs 33% (p=0.037) N=19 N=18 Resolution time: p=0.002
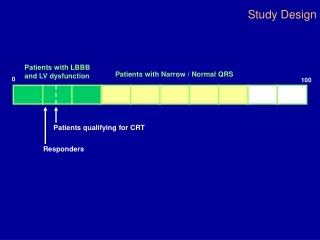
130 patients attending the ED for CPE • Randomized to • O2: n=65 • NIPSV: n=65 • Primary endpoint: need for intubation • Secondary endpoints: mortality, physiological variables
Intubation rate: 25% vs 20% (p=0.5) • Mortality: 14% vs 8% (p=0.4) • Subgroup analysis: no difference P=0.01
CPAP vs Conventional medical treatment: intubation rates NNT=7
36 patients with CPE and hypercapnia (in the ED) • Randomization to CPAP (n=18) or NIPSV (n=18) • Endpoints: • Endotracheal intubation • Death rate • Resolution time (SpO2>96%, BR<30)
In all types of CPE, CPAP improves oxygenation • In LV diastolic dysfunction, this occurs through a decrease of LV diastolic volume (preload) and in MAP • In LV systolic dysfunction, CPAP both decreases preload and increases LVEF