Download
1 / 14
140 likes | 498 Views
Preoperative Embolization of Brain Tumor with Dural Branch of Internal Carotid artery as Feeding Artery. H Hirohata, Y Takeuchi, K Orito, S Yamashita T Abe*, M Shigemori Department of Neurosurgery, Kurume University Department of Radiology, Kurume University. Introduction.

E N D
Preoperative Embolization of Brain Tumor with Dural Branch of Internal Carotid artery as Feeding Artery. H Hirohata, Y Takeuchi, K Orito, S Yamashita T Abe*, M Shigemori Department of Neurosurgery, Kurume University Department of Radiology, Kurume University
Introduction Most important issues in the surgical treatment of the hypervascular brain tumor is the securing and coagulation of feeding artery. Securing the feeding artery prior to actual tumor resection might be difficult in the tumor had the feeding A From deep surface of the operative field. We performed selective feeder embolization before tumor resection.
Indication of Embolization (1997 – 2009) Large hypervascular skull base tumors with feeding artery from deep surface of the operative field( fed by the ICA dural branch) are indicated for preoperative embolization. n = 22 Sex: Age: Tumor location: Max Tumor size: F:M = 17 : 5 31 – 72 (mean 50.95) years Petroclival 17 Sphenoid ridge 3 Olfactory groove 2 30 – 72 (mean 45.7) mm
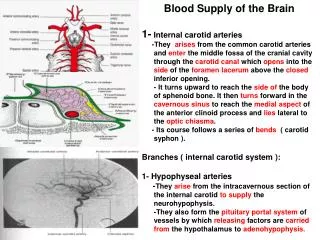
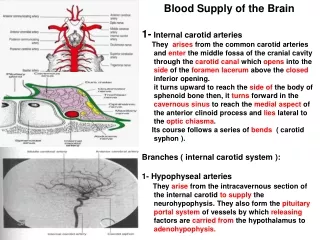
Diagram of the Arteries Arising from the Cavernous Segments of the ICA Meningohypophyseal trunk ( MHT) 6: Medial & Lateral dorsal Clival Artery 7: Marginal Tentorial Artery Infero lateral trunk (ILT) 3: Anterior branch 4: Posterior branch Robinson DH et al:AJNR20: 1061-67, 1999
Feeding artery (22 patients, 29 feeder) Meningohypophyseal trunk ( MHT): 19 dorsal Clival Artery: 13 Marginal Tentorial Artery: 6 Infero lateral trunk (ILT): 7 Posterior branch: 7 Ethomoidal artery: 3 Anterior ethomoidal A:1 Posterior ethomoidal A: 2
Surgical Procedure Embolization was performed within 1-3 days before surgical resection under the local anesthesia and systemic heparinization using routine Trans-femoral technique. 2 or 1.7F microcatheter (FAS Tracker 10 or SL-10) and hydrophilic shapable micro guidewire (Transend floppy, Synchro 14) were used . According to the anatomical relationship of the origin of the feeding artery to the parent A, Micro catheter and micro wire were shaped to C, S, J. Particle embolic material (PVA) was used ( 150 – 250μ).
Surgical Procedure To avoid reflux of embolic material, an high-quality DSA test injection of contrast medium was performed to confirm the absence of reflux of CM into the ICA. The PVA suspension (150 – 200μm) was hand-injected in small small aliquots through micro catheter, using a syringe of the same size as for the test injection. The injection of PVA suspension was continuously monitored using DSA or high quality digital subtraction fluoloscopy (DSF) at 30 frame/s, with a 1024 x 1024 matrix, at low dose radiation. To avoid intra tumoral hemorrhage or ischemic cranial nerve neuropathies, more than 150μm in diameter PVA should be used.
ILT (PB) MHT (LDCA) Post OP (2 stage) MRI Blood loss 740 Initial MRI & CAG TAE (PVA)
Post branch of ILT Post OP(2 stage) MRI Blood loss 1450 Initial MRI & CAG TAE (PVA)
Lat dorsal clival A of MHT Post op MRI Blood loss 650 ml Initial MRI & CAG TAE (PVA)
MHT (MTA) Post OP MRI Blood loss 320 ml Initial MRI & CAG TAE (PVA)
Surgical Results 11 10 1 0 2 12 8 290 – 1450 ( 2 stage OP) mean: 468 ml Angiographical result (tumor stein) Disappeared Markedly decreased Decreased Complication of TAE Surgical results Gross total resection Subtotal resection Partial resection Intra OP blood loss
Conclusion We assessed the clinical value of preoperative embolization of the feeding artery with deep surface of the operative field. All endovascular procedures were technically successful without any complication.