Download
1 / 29
300 likes | 760 Views
Cancer Pathology and Biomarker Reporting. Cancer Surveillance Branch Division of Cancer Prevention and Control National Center for Chronic Disease Prevention and Health Promotion October 1, 2014. National Center for Chronic Disease Prevention and Health Promotion.

E N D
Cancer Pathology and Biomarker Reporting Cancer Surveillance Branch Division of Cancer Prevention and Control National Center for Chronic Disease Prevention and Health Promotion October 1, 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control
Cancer Pathology Reporting Standards • North American Association of Central Cancer Registries (NAACCR) Volume V: Pathology Laboratory Electronic Reporting (based on HL7 v.2.5.1 and v2.3.1)
NAACCR Volume V Specification • OBR-4: Universal Service ID
NAACCR Volume V Specification • OBR-4: Universal Service ID
NAACCR Volume V Specification • OBX-3: Observation ID
Sample HL7 Message OBR|1||22222222222|^^^488136^H+E Histology w/Stains^L|||201309191229||||||LEFT NOSE TIP^^CD- 10001293|||1902001837^TOMAR^RASHMI^^^^MD^^^^^^NPI|||||800^735^4087||||F||||||239.2^Neoplasms of unspecified nature of bone, soft tissue, and skin^IC9| OBX|1|TX|22633-2^Path report.site of origin^LN^502000^MATER^L||Material submitted:.PART A: Shave Biopsy, Left, Nose Tip||||||F|||20130923195248|34D0655205^LabCorp RTP^CLIA||| OBX|2|TX|22637-3^Path report.final diagnosis^LN^502004^FDIAG^L||*** Diagnosis:A. BASAL CELL CARCINOMA, NODULAR TYPE.THE DEEP AND LATERAL MARGINS ARE INVOLVED.||||||F|||20130923195251|34D0655205^LabCorp RTP^CLIA||| OBX|3|TX|19139-5^Pathologist name^LN^502006^SIGNED^L||Electronically signed:.A. LEENA LOURDURAJ||||||F|||20130923195253|34D0655205^LabCorp RTP^CLIA||| OBX|4|TX|22634-0^Path report.gross observation^LN^502007^GROSSD^L||Gross description: .A. Received in formalin is a piece of skin measuring 0.4 x 0.3 x 0.1 cm which is inked, and submitted in toto in 1 cassette.||||||F|||20130923195254|34D0655205^LabCorp RTP^CLIA||| OBX|5|TX|22635-7^Path report.microscopic observation^LN^502008^MICROD^L||Microscopic: .A. Dermal nodule composed of nests of atypical basaloid keratinocytes surrounded by a myxoidstroma. Peripheral palisading, individual necrotic keratinocytes and mitotic figures are present.||||||F|||20130923195255|34D0655205^LabCorp RTP^CLIA|||
Sample HL7 Message OBR|1||999714211|48807-2^Bone marrow aspiration report^LN^6^Bone Marrow Morphology^L|||20111005120000|||||||||^PHYSICIAN^REFERRING|^^^^^555^5555552||||||||F|||||||99999999&Alexa&Liliyana&UNKNOWN&M.D.&&&&UNKNOWN OBX|1|TX|22633-2^Nature of Specimen^LN|1|Bone marrow||||||F|||20111017105722 OBX|2|TX|22634-0^Gross Pathology^LN|1|1) Core: Received in formalin is a core of firm brown bony material measuring 1.0 x 0.2 x 0.2cm entirely submitted in 1 cassette following decalcification. 2) Clot: Received in formalin, clotted material measuring 2.0 x 2.0 x 1.5cm in aggregate, entirely submitted in 1 cassette. 3) Number of slides received: Ten||||||F|||20111017105722 OBX|3|TX|22635-7^Microscopic Pathology^LN|1|Hypercellular marrow for age (70-80%) with maturing trilineage hematopoiesis. The M:E ratio is within normal limits. There is no increase in mononuclear blast-like cells, accentuated paratrabecular immaturity, or abnormally localized immature precursors noted. Megakaryocytes are increased in number and exhibit cytologicatypia. They are pleomorphic, including megakaryocytes with "cloud-like" and hyperchromatic nuclei and they are arranged in tight clusters. No significant lymphoid or plasma cell infiltrates are noted. Reticulin: Diffuse, moderate to marked increase in reticulin fibers. Trichrome stain: focal collagen fibrosis. Iron: Stainable iron is not observed on tissue sample.||||||F|||20111017105722 OBX|4|TX|22637-3^Final Diagnosis^LN|1|1) Hypercellular marrow with maturing trilineage hematopoiesis, increased atypical megakaryocytes, diffuse moderate to marked reticulin fibrosis and focal collagen fibrosis, consistent with primary myelofibrosis (PMF). 2) No increased CD34 positive blasts detected.||||||F|||20111017105722
Cancer Biomarker Reporting National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control
Tests Collected for CER Activities • BCR-ABL/BCR-ABL2: • Cytogenetic analysis • FISH • Qualitative RT-PCR • Quantitative RT-PCR • HER2/ER/PR: • FISH Test Lab Value and Interpretation • CISH Test Lab Value and Interpretation • IHC Test Lab Value and Interpretation • JAK2 • KRAS • Microsatellite Instability • Chromosome 18q: Loss of Heterozygosity (LOH)
CER Questions • Are colorectal cancer patients tested for KRAS and are the results used appropriately to determine treatment? What impact does KRAS testing have on 2-3 year survival among colorectal cancer patients? • Are women with breast cancer being tested appropriately for HER2, progesterone receptor (PR), and estrogen receptor (ER) status and treated appropriately? • Are chronic myeloid leukemia (CML) patients being tested for the BCR-ABL2 gene and receiving appropriate treatment according to those results?
JAK2 Tests provided by Laboratory B • JAK2 V617F Mutation Analysis • JAK2 Exon 12-14 Mutation Analysis
Sample HL7 Message - Biomarker OBR|1||08522507240|^^^489470^JAK2 Mutation Analysis, Quant^L|||20130318|||||||00000000||^MENDPARA^S|||||800^735^4087|20130328|||F||||||| OBX|1|TX|43399-5^JAK2 gene.p.V617F^LN^489471^JAK2^L||The JAK2 V617F mutation is not detected in the provided specimen of this individual. This result does not rule out the presence of the JAK2 mutation at a level below the sensitivity of detection of this assay, or the presence of other mutations within JAK2 not detected by this assay. This result does not rule out a diagnosis of polycythemia vera (PV), essential thrombocythemia (ET) or idiopathic myelofibrosis (IMF) as the V617F mutation is not detected in all patients with these disorders. Results should be interpreted in conjunction with clinical and other laboratory findings for the most accurate interpretation.||||||F|||20130327173353|34D1008914^LabCorp RTP^CLIA|||
Sample HL7 Message – FISH HER2 Breast OBR|1||482042||||20140312000000|||||||20140318104600||^VanHoose^John||||||20140321152303|||F|||||||^VanHoose^John OBX|1|TX|22633-2^Nature of Specimen^LN||Paraffin Tissue||||||F||||^CLIA # 10D0998082. OBX|2|TX|22636-5^Clinical History^LN||Lesions||||||F||||^CLIA # 10D0998082. OBX|3|TX|22637-3^Final Diagnosis^LN||Negative||||||F||||^CLIA # 10D0998082. OBX|4|TX|33746-9^Results: Probe Set Detail^LN||Results show a HER2 to centromere 17 ratio of less than 2.0 and an average HER2 copy number of <4.0 signals per cell following a HER2 breast FISH protocol. This is a NEGATIVE result according to the 2013 ASCO/CAP guidelines.||||||F||||^CLIA # 10D0998082. OBX|5|TX|33746-9^Results: Nuclei Scored^LN||40||||||F||||^CLIA # 10D0998082. OBX|6|TX|33746-9^Results: Interpretation^LN||Along with fluorescence in situ hybridization (FISH), an H\T\E stained slide was reviewed by a pathologist to identify the target area containing invasive tumor. FISH analysis of 40 interphase nuclei was performed within the marked target area using a dual-probe FISH assay (Abbott Molecular, Des Plaines, IL). Controls performed appropriately. Results show no evidence of HER2 amplification and a HER2/CEP17 ratio of <2.0 with an average HER2 copy number <4.0 signals per tile. This is a NEGATIVE result.\.br\\.br\Reference: Wolff AC, Hammond MEH, Hicks DG, et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer. Arch Pathol Lab Med. doi: 10.5858/arpa.2013-0953-SA.\.br\\.br\Note: This HER2 FISH assay was scored on an automated image analysis platform. Two or more independent areas of tumor were analyzed and the technical results underwent a manual technologist review for quality control purposes.||||||F||||^CLIA # 10D0998082. OBX|7|TX|22638-1^Comments^LN||Please use Automated CPT Code 88367.26 X 2||||||F||||^CLIA # 10D0998082.
Sample HL7 Message - Biomarker OBR|1||07922505310|^^^483200^HER2 Rx FISH Rx HERmark(R)^L|||20130314||||||VE3001155 1/2|00000000|||||||800^735^4087|20130325|||F||||||| OBX|1|TX|18474-7^HER2 Ag^LN^483201^HER2^L||2+||||||F|||20130321174419|34D0655205^LabCorp RTP^CLIA||| OBR|2||07922505310|^^^483200^HER2 Rx FISH Rx HERmark(R)^L|||20130314||||||VE3001155 1/2|00000000|||||||800^735^4087|20130325|||F||||||| OBX|1|TX|31150-6^HER2^LN^483211^H2FISH^L|| . No HER2-neu gene amplification was observed for this specimen as defined by the 2007 ASCO/CAP guidelines. Multiple areas of tumor were evaluated and the ratio of HER2-neu/control CEP17 hybridization signals was determined to be less than 1.80. Unless otherwise indicated, only invasive tumor is considered for scoring. . FISH results should be interpreted in conjunction with clinical evaluation and other prognostic factors such as tumor size, nodal status, histologic grade, patient age, hormone receptor status, and other known risk factors.||||||F|||20130325162652|34D0655205^LabCorp RTP^CLIA|||
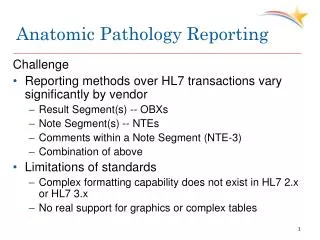
Challenges with collecting Cancer Pathology and Biomarker Data • Laboratories in United States still using text-based reporting • Inconsistent terminologies used across laboratories • Differences in what laboratories include in the reports (genes tested, probes used, qualitative data, quantitative data, etc.) • Test names are not standardized across laboratories • NAACCR Volume V standard may not be able to handle all biomarker data adequately • Data collection is very labor intensive without standardization and use of automated electronic methodology
College of American Pathologists (CAP) Cancer Pathology Protocols and Biomarker Templates
CAP Electronic Cancer Checklists (eCC)and Biomarker Templates • SNOMED-CT used to encode the eCC • CAP Cancer Biomarker Templates need to be coded using LOINC and/or SNOMED-CT • Testing use of Integrating the Healthcare Enterprise (IHE) Structured Data Capture (SDC) to capture and report data included in the eCC and Cancer Biomarker Templates at 2015 IHE NA Connectathon in January 2015
Thank you! Sandy Jones, CDC Public Health Advisor 770-488-5689 sft1@cdc.gov The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control