Download
1 / 56
590 likes | 1.42k Views
Learn about the pathogenesis and management of chronic pancreatitis with surgical and non-surgical approaches. Explore indications, options, and outcomes to enhance patient care and quality of life.

E N D
Chronic Pancreatitis Management Strategies Dr Vidhyachandra Gandhi DNB (GI Surgery), DNB (Gen Surgery), MNAMS Gastrointestinal & HPB Surgeon Ruby Hall Clinic Pune JASICON 2017
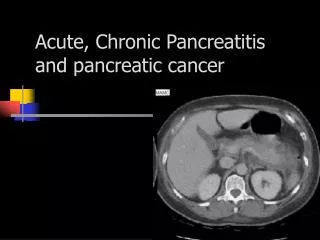
Chronic Pancreatitis Introduction : “ Disease of uncertain pathogenesis , unpredictable clinical course and unclear treatment. It is a chronic inflammatory process leading to irreversible destruction of exocrine tissue , fibrosis and a loss of endocrine function” Two main causes in India are : Alcohol abuse Tropical (Idiopathic) pancreatitis
Chronic Pancreatitis Aetiopathogenesis of Pain : Ductal Hypertension Normal PD pressure 8-12 cm H2O Pressures in Ch.Pan. – 33.4 cm H2O Bradley - 35.4 + cm H2O (controls 14.5 + 1.8 cm H2O) Okazaki - 44.9 mm Hg in minimal pancreatitis Okazaki K, et al Scand j Gastroenterol 1988 Charles F.Frey Advances in Surgery 1995
Aetiopathogenesis of Pain : Perineural and Neural inflammation Inflammatory cells Diameter Pancreatic nerves Neuroimmune interaction Number Perineurium damaged Neurotransmitters Ductal and parenchymal HTN Compartment- like syndrome. Pancreatic pseudocyst & Pancreatic ischemia. Duodenal / CBD obstruction
Chronic Pancreatitis - Pathogenesis Tyler Stevens et al Am J Gastroenterol 99(11):2256-2270, 2004.
Chronic Pancreatitis Medical therapy
Chronic Pancreatitis Endoscopic Therapy: Indications: 1. Dominant stricture in the Pancreatic head with upstream dilatation Major problems: 1. Frequent stent changes 2. Potential ductal alterations 3. Bleeding 4. ERCP Pancreatitis 6. Retroperitoneal perforation J.E.M. Cunha et al Pancreatology 2004;4:540–550 Horst Neuhaus GASTROINTESTINAL ENDOSCOPY Volume 63, No. 1 : 2006
Chronic Pancreatitis Surgical management Indications : Unchanged Pain , Complications ,Malignancy Selection criteria : unchanged Duct anatomy and parenchymal morphology Surgical Options : Changed “Lack of understanding of pain mechanisms has contributed to the difficulty in choosing the best method of treatment”
Chronic Pancreatitis Surgical management • Indications for Surgery: • Chronic pain that responds inadequately to non surgical therapies • Effects of progressive fibrosis on neighboring structures • - Symptomatic duodenal obstruction • - Persistent common bile duct obstruction • - Symptomatic colon obstruction
Chronic Pancreatitis Surgical management 3.Effects of ductal rupture - Persistent large or symptomatic pseudocyst - Pancreatic fistula - Pancreatic ascites 4.Vascular complications - Splenic vein thrombosis with Sinistral portal HTN - Pseudo Aneurysms 4. Suspected pancreatic cancer Unresponsive to non surgical management
Chronic Pancreatitis Surgical management Aim of Surgical treatment: 1. Better long term outcome 2. Preservation of exocrine and endocrine function 3. Improvement of patient quality of life 4. Easy to perform 5. Low morbidity and mortality.
Chronic Pancreatitis Surgical management Resectional procedure Drainage procedures Frey (LR-LPJ) Beger procedure (DPPHR) PD PPPD Distal Pancreatectomy Total Pancreatectomy Duval’s Puestow – Gillesby procedure Modified Puestow’s
Chronic Pancreatitis Drainage procedures Modified Puestow’s
Chronic Pancreatitis Drainage procedures: Modified Puestow's: Initially provides pain relief in 75%-80% Preservation of pancreatic tissue – function Low surgical morbidity and mortality Failure : Pain relief is short lived because of 1. Failure to open duct to duodenum 2. Failure to address disease in the duct of Santroni, duct of uncinate and tributary ducts to these structures and duct of wirsung
Chronic Pancreatitis Drainage procedures: Mucosa to mucosa apposition Single Vs two layer anastomosis Interrupted Vs Continuous sutures Length of ductal decompression: < 6 cm of length anastomosis - less successful less pain relief Diameter of duct – influence the ability to perform LPJ and effect long term pain relief.
Chronic Pancreatitis Resectional procedures: Indications for resection: 1.Small duct disease < 5 mm 2.Inflammatory mass - Pancreatic head is the “Pacemaker” of pain 3.Suspicion of malignancy
Chronic Pancreatitis Hybrid (resection + drainage) procedure: Frey’s (LR- LPJ) - All the three ducts in the head are decompressed - safe - easy to perform - Pain relief is comparable with PPPD and Beger’s procedure - Contraindicated - suspicious of cancer
Chronic Pancreatitis Frey (LR-LPJ)
Complications Pseudocyst CBD obstruction Duodenal obstruction Pancreatic ascites Pancreatic pleural effusion Splanchnic venous obstruction Visceral artery aneurysms
Complications of Chronic pancreatitis Pseudocyst • 20 – 40% • unlikely to resolve • surgical drainage • PD dilated – internal • drainage of the cyst • must be associated • with LPJ
Complications of Chronic pancreatitis Pseudocyst CBD obstruction Duodenal obstruction Pancreatic ascites Pancreatic pleural effusion Splanchnic venous obstruction Visceral artery aneurysms
Chronic pancreatitis related common bile duct stricture Diagnostic Evaluation Serum alkaline estimation US abdomen / Endo ultrasonography CT Scan ERCP/MRCP
Chronic pancreatitis related common bile duct stricture • Operative indications: • Cholangitis • Morphologic evidence of hepatic changes suggestive of • biliary cirrhosis • Progressive dilation of CBD and CHD • Persistent jaundice or elevation serum bilirubin for a month or more • Persistent elevation of Alk.Phos. three times normal for longer than 1 month • Inability to rule out cancer Charles F.Frey :Advances in surgery 1999
Operative selection for biliary stricture 1. Type of biliary drainage 2. Pancreatic drainage / resection Type of drainage: Choledochoenterostomies Endoscopic stent placement – seriously ill and unfit for surgery
Operative selection for biliary stricture Type of drainage: Choledochoenterostomies - Choledochoduodenostomy - Sump syndrome and cholangitis - development of duodenal obstruction - peripancreatic sclerosis may extend above the duodenum Choledochojejunostomy; results are good - clinically and improvements in biochemical parameters
Case CT Scan ERCP
Chronic pancreatitis related common bile duct stricture Chronic pancreatitis with jaundice MRCP Biliary stricture Cholangitis present Without Cholangitis Biliary stenting Pain associated with PD dilatation Suspicion of Ca. Pain present PD Biliary & pancreatic duct drainage Biliary enteric drainage
Complications of Chronic pancreatitis Duodenal obstruction • 1-2 % • common in patients with biliary obstruction • inflammation; fibrosis, pseudocyst • Ist , IInd or IIIrd parts of duodenum - fibrosis • Gastrojejunostomy - prompt relief • Can occur even after LPJ
Complications of Chronic pancreatitis Pseudocyst CBD obstruction Duodenal obstruction Pancreatic ascites Pancreatic pleural effusion Splanchnic venous obstruction Visceral artery aneurysms
Complicated CP – Pancreatic Ascites • 1% incidence ; mortality if untreated - 20-30% • Leak either from pancreatic duct or pseudocyst • USG; high amylase & protein in aspirate • ERCP localizes leak; stenting - ideal • Repeated paracentesis;TPN; Somatostatin for 2-3 wks • Resection / internal drainage of fistula to a Roux loop • Pl.effusions dry once abdominal source is eradicated
Complications of Chronic pancreatitis Pseudocyst CBD obstruction Duodenal obstruction Pancreatic ascites Pancreatic pleural effusion Splanchnic venous obstruction Visceral artery aneurysms
Chronic pancreatitis with Vascular complications Portal hypertension: Splenic vein thrombosis – 31% (4% to 45%) Portal vein occlusion - 4% SMA 1% Bernades .p et al .Dig.Dis.Sci 1992 Splenic Vein Thrombosis : Incidence of varices – 17%- 55% bleed is rare Venous phase of angiography CT Angiography
Chronic pancreatitis with Vascular complications Portal hypertension Treatment: Medical line of management Splenectomy for isolated SVT Additional procedure to treat underlying pancreatic pathology may be performed
Complications of Chronic pancreatitis Pseudocyst CBD obstruction Duodenal obstruction Pancreatic ascites Pancreatic pleural effusion Splanchnic venous obstruction Visceral artery aneurysms Pseudoaneurysm • 10%--17% in ch.Pancreatitis
Pseudoaneurysm • 10%--17% • Splenic artery • Gastroduodenal artery • Pancreaticoduodenal artery Splenic artery pseudoaneurysm
SplenicArteryAneurysm CT Scan CTAngio.
Vascular Embolization Before After Success rate around 67%-100%
Complicated CP - Malignancy • CP predisposes to malignancy • Symptomatic mass in the head of pancreas • With all investigative modalities: (EUS;FNAC) - difficult to differentiate between inflammation & tumour - 15% • Difficult even on the operating table • Frozen section may not help. • Symptomatic mass in the head - Radical resection even if proof of malignancy is lacking
Mass Mass Proximal head Tumour Distal to tumor taped
Distal pancreas with dilated duct Mass Dilated duct with stone Prox Distal