Download
1 / 40

E N D
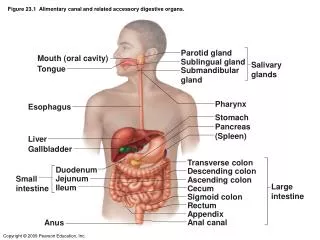
Spleen Anatomy • The spleen lies within the peritoneal cavity in the posterior portion of the left upper quadrant, below the diaphragm and adjacent to the 9th to the 11th ribs, stomach, colon, and left kidney, with its hilum in close approximation to the tail of the pancreas. • The spleen weighs 80-200 grams and 70-180 grams in the normal adult male and female, respectively, approximately 0.2 percent of body weight. • It is not usually palpable, but may be felt in children, adolescents, and some adults, especially those of asthenic build.
Spleen Roles • The spleen is a major lymphopoietic organ, containing approximately 25% of the total lymphoid mass of the body. • The spleen as well as components of the monocyte-macrophage system, can react and enlarge quickly after the onset of infection or inflammation.
Splenic Functions • Site of secondary lymphoid tissue Exposure to blood born antigens, mount immune response “Innate and adaptive” Removal Ab coated RBCs/Platelets . • Storage: Reserve of mature hematopoietic elements • Hematopoiesis: fetal life – extramedullary • Filtration: Important for encapsulated organisms, cellular debris • Red cell modelling: Pit out inclusions, remove damaged membrane, if RBC damaged/old enough – place to “retire” RBCs
Hypersplenism • Normally, about one-third of the platelet mass is sequestered in the spleen, where it is in equilibrium with circulating platelets. • Splenic sequestration of platelets can be increased to 90 percent in cases of extreme splenomegaly. • Patients with cirrhosis, portal hypertension, and splenomegaly may have significant degrees of "apparent" thrombocytopenia (with or without leukopenia and anemia), but rarely have clinical bleeding, since their total platelet mass is usually normal
Hyposplenism and asplenia • Splenic functions are lost when congenitally absent spleen, surgically removed, atrophied following repeated infarction (eg, sickle cell disease), or following splenic artery thrombosis. • Splenic function is reduced in the neonate and may be abnormally reduced (called hyposplenism or functional asplenia) when it is engorged with blood (eg, splenic sequestration crisis associated with sickle cell disease, malaria, splenic vein thrombosis), or infiltrated (sarcoidosis, amyloidosis, tumors, cysts). • Functional asplenia has been described in autoimmune disease, celiac disease, and inflammatory bowel disease.
Infective: Brucellosis, EBV and CMV infections, leishmaniasis, malaria, viral hepatitis • HemolyticAnemias: Thalassemia, sickle cell anemia, hereditary spherocytosis, autoimmune hemolyticanemia • Hepatic diseases and venoocclusive disorders of hepatic veins and portal system: Cirrhosis, hepatic/portal/splenic DVT. • Autoimune Disorders: SLE, Felty syndrome, sarcoidosis, inflammatory pseudotumor of the spleen • Metabolic disorders: Amyloidosis, Gaucher dis. • Others: Cysts, infarction.
Malignant Tumors Spleen mostly secondary involvement • NHL – most common malignancies • Spleen is the primary site • 10% Hodgkin’s disease • 30% of resected spleens (staging procedure) have (+) histology • Hairy cell leukemia • CLL • Myeloproliferative disorders: PMF, CML, PV, CMML Primary Tumours • Angiosarcoma (early metastatic disease; aggressive with rapid growth; spontaneous splenic rupture and hemolytic anemia) Benign Tumors (Hemangioma; Hamartoma; Lymphangioma)
Malignant lymphomas accounted for a relevant, yet probably underestimated, number of splenomegaly. • In patients in which splenomegaly remains “unexplained,” lymphomas account for the leading cause (35-57%) • The spleen may be involved by lymphoid neoplasms during their dissemination as a secondary lymphoid organ. • It rarely represents the exclusive site of the lymphomatous burden. • Nearly 80% of patients presenting with a suspect SL are diagnosed with SMZL or SL-u.
Lymphomas commonly/typically presenting as splenic lymphoma • SMZL • SL-u Splenic diffuse red pulp B-cell lymphoma HCL variant • HCL • LL • B-PLL • T-LGL • Hepatosplenic T-cell lymphoma Primary splenic presentations of nodal lymphomas • MCL • FL • DLBCL • Micronodular T-cell/histiocyte-rich large B-cell lymphoma
How TO Diagnose ? * Good clinical, Laboratory, radiological & Pathological tests are required to get a diagnosis of splenic involvement by lymphoma. * Trying to avoid splenectomy for diagnostic purposes.
1. Full clinical H/O & Examination • The presence of pathologic conditions, such as chronic hepatitis C & B virus infection, autoimmune disorders (eg, SLE, autoimmune thyroiditis), previous therapies with immunosuppressive agents or tumor necrosis factor blockers • B-symptoms • Sore throat, fever, malaise • Symptoms of a rapid and/or massive spleen enlargement, such as left-flank pain and feeling of abdominal fullness.
2. Lab tests • CBC& PB film: PB counts may be normal or display slight to marked lymphocytosis with or without cytopenia (mostly anemia and thrombocytopenia) of variable degree, presence of abnormal circulating lymphocytes, parasites, RBCs changes • Hepatitis, HIV, CMV, EBV • β 2-microglobulin and lactate dehydrogenase,known surrogates of the neoplastic burden • serum M component • Coomb test should be consistently checked because of their high prevalence in lymphomas
3. Radiological review • With unexplained splenomegaly; Ultrasound (US) imaging of the abdomen and whole-body CT scan are mandatory in all patients. • As the “gold standard” investigation for clinical staging of lymphomas, whole-body CT scan allows determining whether the suspected lymphoproliferative disorder is confined to the spleen or it involves other nodal and/or extranodal • PET scan
4. Bone marrow aspirate & biopsy • The BM represents the most easily accessible tissue for the histopathologic analysis. • Is an invaluable source of fresh cells for immunophenotypic, biomolecular, and cytogenetic characterization. • BM evaluation represents the diagnostic “gold standard” & a conclusive diagnosis can be reached in several lymphoid neoplasms presenting as SLs (HCL, T-LGL, and B-PLL ) • BM assessment makes it possible to reach an accurate diagnosis in most cases of MCL, HSTL, LPL, and SMZL, even in the absence of lymph node or spleen assessment
5. Histo-pathological Tissue diagnosis • Lymph node biopsy is warranted once detected & present. • Always resort to diagnostic splenectomy when neither PB examination nor BM assessment highlights the presence of abnormal clones or no lymph nodes cud detected (SMZL, HCL). Lymphoma/leukemia — 57 % Metastatic carcinoma/sarcoma — 11 % Cyst/pseudocyst — 9 % Benign/malignant vascular neoplasm — 7 %
General indications for splenectomy • Diagnostic isolated splenic pathology • Therapeutic alleviate symptoms Massive splenomegaly (adults generally) Refractory ITP, hemolyticanemia Splenic rupture (trauma), NHL • Incidental (injury during surgery) • Surgical procedure in that area requires taking the spleen out to facilitate access or as part of an “en bloc” resection
Splenectomy for Hematologic Diseases • Alleviates symptoms • Corrects hematologic abnormalities • Staging & Diagnosis • Rarely cures the disease Indication of Splenectomy • Red Disorders (HS, AIHA, thalassemia, SCD) • Platelet Related Indications (ITP) • White Cell – Disorders (CLL, HCL, NHL, HD) • Bone Marrow disorders (IMF, MPD)
Other Indications of splenectomy Miscellaneous disorders and lesions a. Infections/abscess b. Storage diseases/infiltrative disorders i. Gaucher's disease ii. Nieman-pick disease iii. Amyloidosis c. Felty syndrome's d. Sarcoidosis e. Cysts and tumors f. Portal Hypertension g. Splenic artery aneurysm h.Splenic vein thrombosis i. Trauma, rupture, surgical maneuver.
Postsplenectomy complications • Atelectasis, pneumonia, effusion (left side) • Hemorrhage (mostly with laparoscopic) • Intraabdominal abscess (LUQ) • Pancreatitis or fistula formation • The presence of Howell-Jolly bodies in circulating red cells, increased numbers of target cells and misshaped red cells & red cells with reduced deformability • Mild degrees of thrombocytosis & leukocytosis. • DVT • PVT • Hemolytic anemia or myeloproliferative diseases with splenomegaly • Sepsis with encapsulated organisms, especially in children. • Postsplenectomy sepsis (PSS)
Postsplenectomy Sepsis • A fulminant and rapidly fatal illness that complicates bacteremic infections with encapsulated pathogens ( Streptococcus pneumoniae, Haemophilus influenza, and Neisseriameningitidis) in asplenic individuals which are normally cleared from the circulation by the spleen • Anatomic or functional asplenia is also a risk factor • Incidence 1/175 patient-years in children, and 1/400-500 patient-years among adults
The incidence of this syndrome is highest in children who had splenectomy in infancy and in splenectomized lymphoma patients who have received combined chemotherapy. • The highest risk of PSS occurs during the first few years following splenectomy but has been documented as late as 20 years later. • The risk of infection is highest during the 90 days following splenectomy, occurring in 10% of splenectomised patients • Hazard of infection was 4.6-fold higher from 91-365 days following splenectomy and 2.5-fold higher >365 days following splenectomy compared with the general population.
Prevention • Avoid splenectomy (if possible) • Immuniztion • Prompt & rapid use of broad spectrum Antibiotics with fever & suspected sepsis
What To Do Prior Elective Splenectomy???What is the Situation of Traumatic or Unpredictable Splenectomy ???
Vaccines should be administered at least 14 days prior to scheduled splenectomy. • If this is not possible, these immunizations can be given after the 14th postoperative day. • Post vaccination immunization titers were not significantly different from control patients. However, opsonophagocytic function of the antibodies was diminished in patients vaccinated before the 14-day point. • In patients undergoing immunosuppressive chemotherapy or radiotherapy, immunization should be delayed for at least 3 months after completion of therapy
Pneumococcal vaccine • Polyvalent polysaccharides antigens that stimulated antibody response. • Should start 2 weeks before splenectomy or once applicable, • Antibody titers appear to decline quickly; splenectomised children & adults have to receive reimmunization with one dose of PV 5 years after the initial immunization
Hemophilus Influenza Vaccine • Haemophilusinfluenzae type B (Hib) conjugate vaccine. • Individuals over age 5 are almost always immune to Hib, even if they have not been immunized. • Thus, the majority of asplenic individuals are not at great risk for Hib disease because most already have specific antibody to this organism. • An additional dose of the Hib vaccine can be given to fully vaccinated children undergoing elective splenectomy • a single dose of the Hib vaccine can be given to splenectomized adults who have not been vaccinated previously
Meningococcal vaccine • Splenectomized individuals should be vaccinated with a meningococcal vaccine according to nation-specific recommendations • A meningococcal quadrivalent conjugate vaccine is recommended for asplenic individuals between 2 and 55 years of age • Revaccination against the meningococcus is recommended for splenectomized patients
Influenza vaccine • Although there are no data regarding the risk for severe or complicated influenza among asplenic individuals, influenza is a risk factor for secondary bacterial infections, such as pneumococcal pneumonia, that can cause severe disease among such patients
Antibiotic prophylaxis 1. Daily antibiotic prophylaxis 2. Empiric antibiotic therapy for fever
Daily Oral Antibiotic prophylaxis • Daily antibiotic prophylaxis in splenectomized individuals was demonstrated to reduce the incidence of infection by 47 % and mortality by 88 % in the splenectomised children compared to those did not receive prophylaxis. • Lifelong penicillin prophylaxis in high-risk individuals (defined as those less than 16 or more than 50 years of age, and those with an inadequate response to pneumococcal vaccination)
Oral Antibiotic prophylaxis • In Children daily prophylaxis with oral penicillin or amoxicillin • First-generation cephalosporins may be used in patients with non-urticarial rash reactions to penicillin (not in patients with a history of anaphylaxis to β-lactam agents). • In adults; the incidence of pneumococcal bacteremia is low, the efficacy of indefinite penicillin prophylaxis for adult patients is debated.
The increased incidence of penicillin-resistant pneumococci, particularly of highly resistant isolates, also threatens the efficacy of current penicillin prophylaxis regimens. • lifelong daily prophylaxis may be considered in survivors of an episode of pneumococcal postsplenectomy sepsis and in highly immunocompromised individuals
Antibiotics for fever • Asplenic individuals, especially those who no longer take penicillin on a daily basis, must recognize that any febrile illness, and should self-medicate with high-dose oral antibiotics. • These patients should have prescribed (and replaced when out-of-date) antibiotics on hand and take them immediately • Then the patient should proceed without delay to the nearest urgent care facility for evaluation and further therapy.
Antibiotic Choice ?? • Recommended oral antibiotics for coverage of S. pneumoniae and H. influenzae include: • Oxicillin-clavulanate • Cefuroximeaxetil • Extended-spectrum fluoroquinoloneslevoflxacin, Moxifloxacin (adults or adolescents only)
Critically ill Cases • Appropriate diagnostic evaluation. • Receive empiric broad-spectrum parenteral therapy such as Vancomycin and 3rd generation cephalosporis/fluoroquinolnes. • In patients who fail to improve following the initiation of an empiric regimen, a resistant organism should be considered (eg, highly penicillin-resistant S. pneumoniae, fluoroquinolone-resistant S. pneumoniae) and the regimen should be adjusted if resistance is thought to be likely. • Poor clinical response despite appropriate therapy is seen in patients with advanced sepsis complicated by refractory hypotension and DIC.