Download

1 / 64
640 likes | 964 Views
Chromosome Abnormalities and Their Molecular Correlates in Acute Leukemia. SAI-JUAN CHEN State Key Laboratory of Medical Genomics Shanghai Institute of Hematology, Ruijin Hospital Shanghai Second Medical University(SSMU). Development of Classification of Acute Leukemia.

E N D
Chromosome Abnormalities and Their Molecular Correlates in Acute Leukemia SAI-JUAN CHEN State Key Laboratory of Medical Genomics Shanghai Institute of Hematology, Ruijin Hospital Shanghai Second Medical University(SSMU)
Development of Classification of Acute Leukemia 1976 French-American-British (FAB) Cooperative Group proposed classification of acute leukemia based on morphologic criteria that were subsequently refined in 1981 and 1985 1986 Morphologic, immunologic and cytogenetic (MIC) classification was introduced. Recognition of importance of cytogenetics in the diagnosis and treatment of acute leukemia 2001 World Health Organization (WHO) classification recognized new clinically relevant molecular genetic lesions
4 5 6 4 5
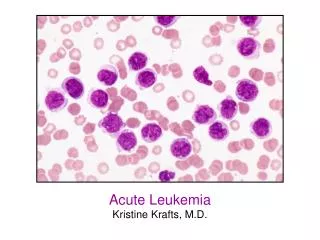
Acute leukemia of ambiguous lineage • Undifferentiated acute leukemia • (HLA-DR, CD34, CD38) • Bilineal acute leukemia • (dual population of blasts) • Biphenotypic acute leukemia • (co-expression of myeloid and other lineage antigen)
白血病染色体易位 Most of the fusion genes involved in AL translocations are transcription factors (TFs): abnormalities in lineage commitment and differentiation Look AT. Science, 278: 1059
More study should be done • Molecular characterization of undetectable abnormalities on the cytogenetic level • Characterization of additional chromosomal or molecular genetic abnormalities [e.g. t(11;17)] in the well-defined favorable cytogenetic group may influence clinical outcome • Characterization of cooperating genetic abnormalities may affect treatment response in stepwise leukemogenesis
Hematopoiesis: a model of systems biomedicine Common Myeloid Progenitor (CMP) Hematopoietic Stem Cell (HSC) Common Lymphoid Progenitor (CLP) GMP EMP Important players: Hematopoietic stem cells, cytokines, microenvironment
Red cells Platelets 造血生成调节的关键因子: 转录因子 TFs are primordial in regulating the switch of the hematopoietic organ, the lineage commitment and the differentiation of HSCs and progenitor cells TF genes related to hematopoiesis are evolutionarily well conserved from the zebrafish to human KO animals for some of these TFs exhibit phenotypes of hematological disorders
Chromosomal translocations and gene mutations in leukemias Most of the fusion genes involved in AL translocations are transcription factors (TFs): abnormalities in lineage commitment and differentiation Look AT. Science, 278: 1059
Nodal points in controlling hematopoiesis: tyrosine kinases KO mice for hematopoiesis related PTKs often show deficiency in blood formation PTKs Hematopoiesis related PTKs are essential factors in determining growth and survival of HSCs and progenitor cells
Chromosomal translocations and gene mutations in leukemias BCR-ABL, a model of activation of protein tyrosine kinase (PTK) in leukemo-genesis: growth and survival advantages
白血病基因组解剖学计划 (L-GAP) 必要性:约50%的白血病患者无染色体异常,即使有特异的基因异常也不足以产生典型的白血病(如AML-M2b的AML1-ETO; CML的BCR-ABL);大多数白血病患者无病生存期远不理想。 大规模系统性候选基因(造血系统转录因子和胞浆信号分子尤其是酪氨酸激酶)的基因突变检测及蛋白质功能研究。 基于药物靶点的高通量筛选库(传统中药天然药物库,组合 化学合成物库)和基于信号传导途径知识的药物设计/组合。
白血病遗传学基础: 白血病基因组解剖学计划 (LGAP) Genes re-sequenced: TFs: AML-1, CBFβ, C/EBPα, GATA1 , GATA1p , GATA2 , GATA2p , GATA3 , MYB , PU.1, … Signaling molecule: PDGFRa, PDGFRb, c-KIT/SCFR, FLK2/FLT3, NRAS, KRAS, ICSBP, NOTCH1, NOTCH2, NOTCH3, …
白血病遗传学基础: 白血病基因组解剖学计划 (LGAP) Two-hits hypothesis
Acute Myeloid leukemia with recurrent genetic abnormalities in classification of WHO • AML with t(8;21);AML1-ETO • AML with abnormal marrow eosinophilia and inv(16) or t(16;16);CBF-MYH11
M2b急性髓系白血病靶向治疗研究 • 12-20% of AML • 40% of AMLM2 • t(8;21) (q22;q22) • AML1-ETO 融合基因
t(8;21) 染色体易位AML-M2患者发生高频率肿瘤基因 c-Kit “功能获得性” 突变[26/54(48.1%)] 和/或异常表达(>80%)
In three cases during complete remission,only AE, but not mC-kit, could be persistent mC-kit should be a subsequent event on the basis of t(8;21), demonstrating a stepwise model in leukemogenesis
Stepwise leukemogenesis and potential of targeted therapy in AML with t(8;21)/AML1-ETO h i t 1 h i t 2 ? t r a n s c r i p t i o n f a c t o r e . g . , A M L 1 - E T O P T K m u t a t i o n C - K I T m e d i a t o r T G F d e c r e a s e C - K I T t r a n s c r i p t m e d i a t o r m e d i a t o r m e d i a t o r P T K a c t i v i t y G - C S F R N c o R - m S i n 3 - H D A C B C L - 2 C - K I T c - J U N , T I S 1 1 b e v a d i n g i n h i b i t i o n o f p r o l i f e r a t i v e a n d a p o p t o s i s d i f f e r e n t i a t i o n s u r v i v a l a d v a n t a g e
control SIH10 2μM,24h SIH10 2μM,48h Oridonin (SIH 10) Screening for AML1-ETO oncoprotein targeted agents based on natural compounds from TCM
SIH10 (mM) AML1-ETO Time (hrs) AML1-ETO Procaspase 3 Casp 3, p17 PARP Casp 9 Cytoplasmic cyt C Control SIH10 2, 12h 2 μM,24h β-Actin SIH10, extracted from a TCM herb: targeted therapy for t(8;21) leukemia?
Stepwise leukemogenesis and potential of targeted therapy in AML with t(8;21) /AML1-ETO: Is C-KIT a therapeutic target for Imatinib? PNAS 2005, 102:1104
Differentiation inhibition Apoptosis inhibition t(8;21) 白血病:异常转录因子/酪氨酸激酶双重靶点? SIH10 STI571 HD Ara-C PTK TGFβ 2, gene mutation 1, t(8;21)(q22;q22) AML1-ETO Tyrosine kinase G-CSF, G-CSFR Bcl-2 P14(ARF) AML1, G-CSF(?), GM-CSF, C/EBPα, PU.1 TIS11b c-JUN proliferation Upregulation or high level HD: high dose t(8;21) leukemia Downregulation or inhibition
Characteristics of 5 Subtypes of APL Chromosomal t (15;17) t (11;17) t (11;17) t (5;17) dup aberration (q22;q21) (q23;q21) (q13;q21) (q35;q21) (17) (q21.3q23) Frequency >95% 1~2% rare rare rare Fusion gene PML-RARa PLZF-RARa NuMA-RARa NPM-RARa STAT5b-RARa 100% 100% yes yes yes RARa-PML RARa-PLZF RARa-NuMA RARa-NPM RARa-STAT5b 60~70% 100% no yes no Nuclear in 100 micro speckles, localized in microspeckle sheet like microspeckle localization which maybe microspeckles pattern aggregation pattern, maybe localized in be localized cytoplasm in cytoplasm Response to ATRA good no, may respond good yes no to ATRA+G-CSF Chemo good no, may respond to chemo/ATRA Arsenic good, with no PLZF-RARa not known not known not known degradation of degradation PML-RARa
der(17) 15 der(15) 17 急性早幼粒细胞白血病(APL)-多步骤发病 原理和靶向治疗 Tg mice Long latency:12m low penetrance: 20-30%
急性早幼粒细胞白血病(APL)-多步骤发病原理和靶向治疗急性早幼粒细胞白血病(APL)-多步骤发病原理和靶向治疗
急性早幼粒细胞白血病(APL)-多步骤发病原理和 靶向治疗 104 (number) * (57) 2 50 (42) 17 (40.5%) 24 (5) 2 (104) 21 (20.2%) 6 (5.8%) 77 (74.0%) Tg mice with both PML-RARa and FLT3 mutation have early onset disease in most animals
急性早幼粒细胞白血病(APL)-多步骤发病原理和 靶向治疗 FLT3 mutation in only part of APL cases and its disappearance ahead of PML-RARa over remission suggests it as an event after PML-RARa
Paradigm shift: from differentiation to molecular target-based therapy • ATRA differentiation therapy of APL: • Complete remission rate: 85-95% • Post-remission therapy (with chemo): 5 year disease-free survival (DSF) rate: 50% • Mild side effects • Targeting PML-RARa
Arsenic trioxide as treatment for APL: ancient remedy performs new trick • As2O3 in the treatment of relapsed patients after ATRA: • Complete remission rate 80-90% • No cross-resistance to ATRA or • chemotherapy • Mild side effects • Induction of PML-RARa degradation (As) hUbc 9 hUbc 9 a PMLsumolation RING finger B1 B2 coiled-coil NLS Enhancement of PML sumoylation Recruitment of PML and interacting proteins NH2 Ubiquitin-like SUMO peptide COOH K490 K160 PMLdegradation SAE1 b ATO SAE2 SUMO interacting protein sequestration
全反式维甲酸 维甲酸受体 PML RARa SUMO-1 APL细胞 PML RARa PML-RARa 致病蛋白 PML 三氧化二砷 分化 凋亡 ATRA/As2O3对APL协同靶向治疗: 异常转录因子作为靶点
ATRA和As2O3联合治疗初发APL 取得迄今为止成人急性白血病的最好疗效 ATRA+As2O3(n=20) As2O3(n=18) ATRA (n=19) 治疗后 : 治疗前 (%) 累计生存率 月 2003年12月全美血液学大会(ASH)专题报告,并在会新闻发布会上作专题介绍 无病生存情况(随访期:8-30月, 中位随访期:18月)
Study group (n=52, MFU:34m) P=0.00001 Historic control (n=51, MFU:56m) APL成为第一个可治愈的成人白血病 Historic Control: 1998-2001 No difference from the study group in terms of prognostic factors (age, WBC, etc) Tx: ATRA+CT; ATO used for rescue in relapsed patients
Chr.11 der 11 The karyotypes of the patients A B 46,XY,Ph,t (1;11) 46,XY,t (11;12)
A B C Chr 11 Chr 3 b D E F F der(11) Fig 1
HD HOXA9 272 HD 1 HD 272 1 HD PMX1 1 217 1 HOXC11 304 NUP98-HOXA9 1 546 aa HD RD NUP98 Docking site (FG motif) 1 920 578 aa NUP98-HOXC11 1 HD 608 aa NUP98-PMX1 HD 1 Docking site (FG motif) Docking site (FG motif) Docking site (FG motif)
M P N B M B N P 750 bp 500 bp 500 bp 300 bp A B C D Fig 2
PMX1 HDAC1 PMX1 NUP98-PMX1 SRF SRF × FOS FOS SRE SRE Possible molecular mechanism of NUP98-PMX1 in leukemogenesis: recruitment of HDAC1 and transcriptional repression of Fos gene regulated by SRF/NUP98-PMX1 heterodimer
Usually occur in a lineage- specific manner, suggesting a crucial role for MLL fusion partner in determining disease phenotype