Download
1 / 1
10 likes | 148 Views
TREND OF LIPIDS. INTRODUCTION. ENDOCRINE EVALUATION.

E N D
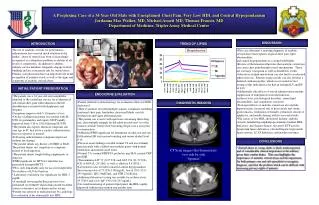
TREND OF LIPIDS INTRODUCTION ENDOCRINE EVALUATION The use of anabolic steroids for performance-enhancement has received much attention in the media; abuse of steroids has been is increasingly recognized as a ubiquitous problem in athletes of all levels of competition. In addition to athletes, military service members frequently engage in body building and are at increased risk for steroid abuse. Primary care physicians have an important role in the recognition of patients at risk as well as the signs and symptoms of anabolic steroid abuse. Hospitalization • Patient referred to endocrinology for evaluation of his low HDL cholesterol. • Their evaluation revealed multiple somatic complaints including exertional chest pain, headaches, decreased libido, erectile dysfunction and vague abdominal pain. • The patient was evasive with questions concerning illicit drug use; after multiple attempts he did admit he took oral “over the counter steroids” before their becoming illegal over a year prior to examination. • Additional PMH significant for intermitant alcohol use and one EtOh related ER visit nausea/vomiting and serum alcohol level 0.18 • Physical exam findings revealed normal VS and an extremely muscled male with a diffuse non-nodular goiter with normal virilization and normal sized testes. • Normal UA, normal FSH/FT4, prolactin, neg HcG, normal CRP and ESR • Transaminitis AST 71 (0-37 U/L) and ALT 154 (21-72 U/L) • CK of 865U/L (25-200), as well as aldolase 8.8 (IU/L) • Laboratories also revealed a marked central hypogonadism: Testosterone total of 73 (250-1100)ng/dL, free of 20.0 (35.0-155.0pg/mL), LH 1.9mIU/mL, and FSH 2.7mIU/mL. • Additional laboratory testing was notable for erythrocytosis 15.7/46.9 and a low IgF-1 90 (106-255 ng/mL) • On serial monitoring of patients lipid panel, the HDL rapidly improved without intervention one months time DIAGNOSTIC IMAGING CT Scan images that demonstrate two side by side “lipomas” CONCLUSIONS • Steroid abuse in young adults is likely under-reported and of considerable clinical importance in the military given their combat duties. This case highlights the importance of anabolic steroid abuse and the importance for both primary care and sub specialists to recognize, diagnose, and treat the problem which can be difficult with increasing privacy rights of patients. A Perplexing Case of a 34 Year Old Male with Unexplained Chest Pain, Very Low HDL and Central Hypogondanism Jordanna Mae Walker, MD, Michael Arnett MD, Thomas Francis, MD Department of Medicine, Tripler Army Medical Center DISCUSSION • This case illustrates a unifying diagnosis of anabolic steroid abuse that explains atypical chest pain, lipid abnormalities, • and central hypogonadism in a young bodybuilder. • Review of the literature illustrates that anabolic steroid use can cause chest pain through several mechanisms. These are coronary vasospasm as well as thrombotic events. • Alterations in lipid metabolism can also lead to accelerated atherosclerosis. Patients using steroids can also develop a dialated cardiomyopathy; which was revealed in later testing of this individual as he had an enlarged LV and EF of 44% • Additionally side effects of steroid administration include suppression of endogenous testicular function, erythrocytosis, psychological disorders, serum lipid abnormalities, and coagulation activation • Prolonged effects of anabolic steroid use also include: hepatotoxicity, increased risk of heart attack and stroke, gynecomastia, virilization of females, premature closure of epiphyses, and needle sharing with its associated risks • The causes of low HDL cholesterol include: anabolic steroids, familial hypoalphalipoproteinemia familial HDL deficiency and Tangier disease, elevated CETP activity, lipoprotein lipase deficiency, elevated hepatic triglyceride lipase activity, LCAT deficiency and insulin resistance INITIAL PATIENT PRESENTATION • The patient was a 34 year old avid weightlifter admitted to the cardiology service for evaluation of sub-sternal chest pain with radiation to the left shoulder/arm associated with diaphoresis and dyspnea. • Symptoms improve with 5-15minutes of rest. • On day of admission patient was treated with SL NTG via paramedics and reports SSCP rapidly improved from 7/10 to 1/10 following SL NTG. • The patient also reports identical symptoms one year ago in SC that led to a cardiac catheterization that was reported as normal. • Following catheterization symptoms improved without any therapy. • The patient denies any history of GERD or RAD. The patient denies rest symptoms or symptoms related to food ingestion. • The patient denies weight lifting supplements or drug use. • PMH significant for HTN for which he was perscribed lisinopril/HCTZ • PE is only remarkable only for an avid weight lifter. No evidence of LV dysfunction • Laboratory evaluation was significant for HDL 3 mg/dL • A treadmill test using the Bruce protocol was performed on 21Mar05 which demostrated excellent exercise toleratnce, no ischemia and no ectopy. • Patient was referred to endocrinology by cardiology for evaluation of his abnormally low HDL.