Download

1 / 52
740 likes | 1.92k Views
An Approach to Fever without a Source in Infants and Children. Authors: Dr. April Kam MD, DTMH, MScPH, FRCPC Parnian Arjmand MSc, MD Candidate Dr. David Goldfarb MD, FRCPC Date Created: December 2012. Learning Objectives. Be able to define Fever Without a Source (FWS)

E N D
An Approach to Fever without a Source in Infants and Children Authors: Dr. April Kam MD, DTMH, MScPH, FRCPC Parnian Arjmand MSc, MD Candidate Dr. David Goldfarb MD, FRCPC Date Created: December 2012
Learning Objectives • Be able to define Fever Without a Source (FWS) • Develop an approach to categorizing and managing a child presenting with fever • Learn about some of the key red flags and special circumstances for children presenting with fever
Caveats… • Need to be aware of local epidemiology • Prevalence of infections can vary dramatically based on geography, season, context of epidemic • Fever Differential Diagnosis can be quite broad– we will only cover most commonly seen entities • Broaden your differential, particularly in immunocompromised children (e.g. HIV, severely malnourished, etc.)
Caveats…(cont’d) • In many countries the epidemiology is changing dramatically due to newly introduced vaccines (e.g. Hib, PCV) and the spread of HIV • Can often see co-infections • e.g. Among < 5 yr olds in Nigeria with confirmed malaria, 9% also had UTI (OkunolaPO et al., 2012)
Caveats… (cont’d) • Very little published data on the management of fever without localizing signs in children in the developing world • Drug resistance rates climbing dramatically in the developing world…
Target Audience • Health care providers working at first level referral centre – primary care hospital • Basic laboratory facilities (e.g. microscopy) and medications available • Need to adapt to your facility based on epidemiology, testing, and antimicrobials available – know the local guidelines!
Main reference • Integrated Management of Childhood Illnesses – Management of a Child with Serious Infection or Severe Malnutrition • https://apps.who.int/chd/publications/referral_care/contents.htm
Definitions • Fever without a Source (FWS) or Fever without Localizing Signs (FWLS) or Fever without a Focus (FWF): • Rectal temperature > 38°C (> 101ºF) in an infant or child w/ a physical exam that does not suggest a focus of infection
Fever • An intrinsic adaptive response that activates the immune system • Is controlled by the hypothalamus • Shortens the length of disease
Etiologies • Infection • Infection • Infection • Other causes much less likely • Inflammation – e.g. Kawasaki disease • CNS disorder – e.g. Hypothalamic dysfunction • Metabolic • Iatrogenic: drugs, immunizations
4 Major Categories for child presenting with fever • Fever due to infection without localized signs – i.e. FWLS (no rash) in > 2 mo • Fever due to infection with localized signs (no rash) in > 2 mo • Fever with rash in > 2 mo • Special Situations/Red Flags • Young infant (7 days - 2 months) – high risk serious bacterial infection • HIV infection • Severe Malnutrition
Differential Dx of Fever with localizing signs (no rash) – cont’d
Special Situations/Red Flags • Young infant – 7 days to 2 months • HIV infected child • Severely malnourished child
Young infant 7 days – 2 months • Presume Serious Bacterial Infection • e.g. Pneumonia, sepsis, meningitis • Show less specific signs • Can present with Fever or Hypothermia • Irregular breathing, jaundice, apnea, grunting, seizure, vomiting, abdominal distension, lethargy, anorexia
HIV infected or potentially infected • HIV infected children have higher risk of sepsis and opportunistic infections • Signs common to HIV infected infants: • Recurrent infections, oral thrush, chronic parotitis, generalized lymphadenopathy, hepatosplenomegaly, persistent/ recurrent fever lasting >7 days, neurological dysfunction, Herpes Zoster, HIV dermatitis • More specific signs: pneumocystic pneumonia, esophageal candidiasis, lymphoid interstitial pneumonia, shingles or Kapsosi sarcoma • Signs common to both HIV infected and non-infected infants: chronic otitis media, persistent diarrhea, failure to thrive
Severe Malnutrition • Definition - edema in both feet or severe wasting and weight for height < -3 SD or <70% • Assume that all severely malnourished children have an infection (regardless of presence of fever) and treat with antibiotics • On exam look for: dehydration, pallor, signs of HIV infection/ local infection, fever, ulcers, skin changes of kwashiorkor
History • Duration of fever • Residence in or recent travel to an area with Plasmodium falciparum (malaria) transmission • Skin rash • Stiff neck or neck pain • Headache • Pain on passing urine (generally child ≥ 3yr) • Ear pain – e.g. pulling on pinna • Immunizations
History (cont’d) • What was the temperature and how was it measured? • Level of activity prior and after onset of fever • Infection(s) during pregnancy or at birth • Ill contacts or recent travel history • Oral intake • Presence of lethargy/ irritability • Presence of cough/ vomiting • Urination frequency/ abdominal pain/ back pain/ new onset of incontinence (e.g. UTI) • Protection of the affected area in deep soft tissue/ bone infection • Underlying medical conditions (e.g. sickle cell disease, urinary tract reflux, etc.)
History (cont’d) - Immunizations • It is particularly important to know if Hib, pneumococcal, meningococcal and/or yellow fever vaccines have been given and are up to date • Nearly all low income countries have now rolled out Hib vaccine • > 18 countries in developing world have also recently introduced PCV • 6 countries in sub-Saharan “meningitis belt” have just introduced new meningococcal A conjugate vaccine • Rapid increase in number of children vaccinated against yellow fever with assistance GAVI • Vaccination with the above conjugate vaccines (i.e. Hib, PCV) dramatically reduces the risk of occult bacterial infection in children presenting with fever without localizing signs
Physical Examination • Always fully undress child • General appearance (alert, playful, irritable, consolable, lethargic) • Oxygen saturations (if available) • Stiff neck • Hemorrhagic skin rash - purpura, petechiae • Skin infections - cellulitis or skin pustules • Discharge from ear/red immobile ear-drum on otoscopy • Severe palmar/conjunctival pallor • Refusal to move joint or limb • Local tenderness • Fast breathing
Physical Examination • Toxic-appearing: • Lethargic: decreased level of consciousness/ poor eye contact, failure to interact with environment or parents • Poor perfusion and cyanosis • Hypo/ hyperventilation • Purpura may be present Woods, CR. Epiglottitis (supraglottitis): Clinical features and diagnosis. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2012.
Physical Examination • Watch for signs of raised intracranial pressure: • Bulging fontanelle • Poor feeding, Vomiting • Headache, Irritability • Papilledema • Lethargy, Seizures • Cushing’s triad: hypertension, widened pulse pressure, bradycardia
Fever 2 months – 3 years • The first step is to determine if the child is toxic looking i.e. septic • If the patient is septic, do septic work up and start antibiotics, fluids, and provide oxygen
Fever 2 months – 3 years • In the non-septic child, the second step is to determine if the fever is due to an infection with or without localized signs by doing a detailed history and physical • If a focus is found, treat accordingly • If no focus is found, investigate as FWLS or Fever without a source
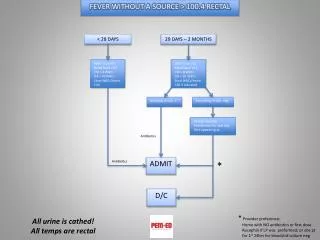
Fever 2 months – 3 years • Example of an institutional algorithm for FWLS in the 2 m – 3 year age group developed for Botswana referral hospital (where there is very low/no malaria, no typhoid, no dengue) is provided on the next page
Algorithm: Fever without a Source – Ages 2 months to 3 years • Child Appears Toxic • Lethargic (not interacting with caregivers/environment) • Poorly perfused (cap refill > 2sec) • Hypoventilating or tachypneic for age Definition: Child between 2 months and 3 years with an axillary temperature > 37.5 and no obvious source of infection after a thorough History and Physical *Normal Rates Age Respiratory Heart 2-12 months <50/min <160/min 1-2 years <40/min <120/min 2-5 years <40/min <110/min 6-8 years <30/min <110/min No Yes Child is HIV positive, CD4 <25% or unknown or child is HIV Exposed and HIV status unknown • Sepsis evaluation • Blood Culture • Urinalysis and Culture • CBC • LP if indicated by symptoms • Consider malaria smear if indicated • Admit to Ward • Start empiric antibiotics-Cefotaxime 50mg/kg/dose 6 hourly No Yes T > 38.5 axillary Yes No Tests: Blood Cx or FBC and then Blood Cultures only if WBC > 15,000 UA and Cx: if Male < 6 mo, Female < 2 yr or T > 40 CXR: if dyspnea, cough/rales LP: if < 15 mo, or associated with seizure and does not meet criteria for simple febrile seizure • No diagnostic test • Paracetemol 15mg/kg/dose • Discharge home • Return if fever > 48 hrs or seems more sick • NO Antibiotics Treatment:- If any diagnostic tests are suggestive of a source for infection treat according to protocol for that diagnosis . However, if no tests are indicated or all test are normal AND If FBC or WBC > 15,000 THEN -> Amox/Clav for 48 hours If FBC or WBC < 15,000 then do not give antibiotics ALL children regardless of whether they are given abx NEED: F/U in 48 hours if still febrile or at any time if they appear more sick & Paracetemol 15 mg/kg/dose
Management – Presumed Septicemia • Treatment • Give benzylpenicillin IV (50 000 units/kg every 6 hrs) or ampicillin 50 mg/kg IM every 6 hrs) plus chloramphenicol (25 mg/kg every 8 hrs) for 7 days • If significant drug resistance to these antibiotics among Gram-negative bacteria, follow the local guidelines for management of septicaemia may be a third-generation cephalosporin such as ceftriaxone (80 mg/kg IV, once daily over 30-60 minutes) for 7 days
Management – Presumed Septicemia (cont’d) • Supportive care • If a high fever of ≥ 39°C (≥ 102.2°F) is causing the child distress or discomfort, give paracetamol (15mg/kg/dose every 4 hours, maximum 5 doses/day ) • Fluid intake and nutritional management • Manage complications including seizures, hypoglycemia, electrolyte abnormalities
Investigations for FWLS – Depending on availability • Blood smear or rapid diagnostic test (RDT) for malaria (if endemic) • LP if signs suggest meningitis (with no signs of raised intracranial pressure, in stable patient) • Blood culture in suspected sepsis • Full Blood Count • Urinalysis/Microscopy • CXR – if pneumonia is suspected
Management 7 day to 2 month old • Investigations: • Check glucose • Do Cultures – Urine and Blood • Do an LP • CXR if available • Management: Oxygen, Fluids, Antibiotics
Management 7 day to 2 month old • Ampicillin (50 mg/kg IM/IV every 6 hrs for 2 days) then oral amoxicillin (15 mg/kg every 8 hrs for 5 days) OR oral ampicillin (50mg/kg PO every 6 hrs on an empty stomach for 5 days) • plus IM gentamicin (7.5 mg/kg once daily) for a total of 7 days of therapy • You may continue IV Ampicillin beyond 2 days if child continues to appear unwell
Management 7 day to 2 month old (cont’d) • If S. aureus is known to be an important cause of neonatal sepsis locally, or signs suggestive of severe staphylococcal infection (e.g. skin pustules), give IM cloxacillin (50 mg/kg every 6-8 hrs depending on age) plus IM gentamicin (7.5 mg/kg once daily)
Management 7 day to 2 month old - Suspected or Confirmed Meningitis • Give IM ampicillin (50 mg/kg every 6-8 hrs depending on age) plus IM gentamicin (7.5 mg/kg once daily). An alternative regimen is IM ampicillin plus IM chloramphenicol (25 mg/kg every 6 hours). • Chloramphenicol should not be used in premature infants and should be avoided in infants in the first week of life • Some centres use third generation cephalosporins
Investigations may include • Glucose (mandatory) • Labs: Hb/ Htc if severe pallor • Electrolytes (generally hypokalemic) • Blood culture • TB investigations • HIV testing, etc.
Management of child admitted with severe malnutrition • Multidimensional management in two phases of stabilization and rehabilitation [see chapter 7 in the WHO manual]
Management of child admitted with severe malnutrition • All severely malnourished children receive • A broad-spectrum antibiotic • Ampicillin (50 mg/ kg IM/IV 6-hourly for 2 days) then oral amoxicillin (15 mg/ kg 8-hourly for 5 days) OR oral ampicillin (50 mg/kg IM/IV for 5 days) over a total of 7 days • Gentamicin (7.5 mg/kg IM/IV) once daily for 7 days If child fails to improve within 48 hours: add chloramphenicol (25 mg/kg IM/IV 8-hourly) for 5 days • Local antibiotic regimen may be different due to different resistance rates
Management of child admitted with severe malnutrition • Measles vaccine if child > 6 mo (not immunized) or > 9 month • Delay vaccination if in shock
Diagnostic Criteria for Urinary Tract Infections • Clinical signs: • Malodorous urine/ hematuria • Abdominal tenderness/ suprapubic pain • Vomiting, irritability, diarrhea • Fever > 38 °C for over 24 hrs • Dysuria, vaginitis/ vulvalitis • Labs: • Urinalysis from suprapubic aspirate or transurethral catheter • Leukocyte esterase • Nitrite • WBC • Culture
Treatment of Urinary Tract Infections • For Oral agents, be aware of local susceptibilities – treatment include: • Amoxicillin/Clavulanate, First generation cephalosporins, Quinolones • If <6months, or septic, require admission and IV Ampicillin & Gentamicin
Other Common Infections • Malaria (see- http://apps.who.int/medicinedocs/documents/s19105en/s19105en.pdf for details) • Varies by severity, endemic species, and resistance patterns • Antimalarial treatment: IM/IV Artesunate first line for severe malaria due to P. falciparum in most regions (pre-referral rectal artesunate an option) • Measles • Two doses of Vitamin A to all children; immediately on diagnosis and within 24 hours
Other Common Infections • Typhoid • Chloramphenicol (25 mg/ kg every 8 hours) for 14 days • If systemic signs/ upset: benzylpenicillin (50 000 units/ kg every 6 hours) for 14 days in addition to chloramphenicol (dosed as above) • Ear infections • Acute otitis media - Amoxicillin (50 mg/kg PO TID) X 7 days • Chronic suppurative otitis media – wicking and topical antibiotic such as chloramphenicol drops if available
Summary • FWS: fever without a specific source in an acutely ill, temp (rectal) > 38ºC (100.4ºF) • Infection is the most common etiology of FWS • There are four categories of infants presenting with fever: young infant with serious risk of bacterial infection, infectious fever without rash, fever due to infection with localized signs, and fever with rash • Management strategies vary depending on geographical area, access to resources, presentation, and infant age • Red flags to watch out for: severely malnourished infant, infant with signs of HIV and young infant (7 days to 2 months)