ANAPHYLAXIS
ANAPHYLAXIS. Prepared by: South West Education Committee. South West Education Committee. Anaphylaxis Protocol. SWEC MEMBERS. Cambridge – Lori Smith Grey Bruce – Andy Whittemore Hamilton – Ken Stuebing, Tim Dodd Lambton – Judy Potter London – Tre Rodriguez Niagara – Greg Soto

ANAPHYLAXIS
E N D
Presentation Transcript
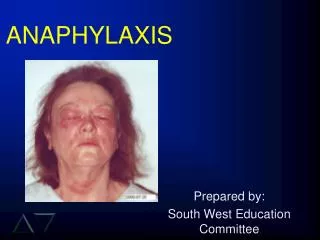
ANAPHYLAXIS Prepared by: South West Education Committee
South West Education Committee Anaphylaxis Protocol
SWEC MEMBERS • Cambridge – Lori Smith • Grey Bruce – Andy Whittemore • Hamilton – Ken Stuebing, Tim Dodd • Lambton – Judy Potter • London – Tre Rodriguez • Niagara – Greg Soto • Windsor – Cathie Hedges • RTN – Peter Deryk
“The Power of 7” Base Hospital Programs • Goal: One single certification for all of SouthWestern Ontario by Fall 2005!! • Recert process same across SW this year. • Notice, all paperwork will say SWEC. • Some information may not be specific to Hamilton BH or Services in our area. • Pictures for data base in one of the stations
OBJECTIVES • Review basic pathophysiology of Anaphylaxis • Review Anaphylaxis. • At the end of this session you should be able to describe and explain: Anaphylaxis and its’ treatment protocols.
ANAPHYLAXIS • An immediate, systemic, life-threatening allergic reaction associated with major changes in the cardiovascular, respiratory and cutaneous systems. • Prompt recognition and appropriate drug therapy are important to patient survival.
A, B, C, … • Assess the patient’s… • Airway (do they have one? Can they maintain it? • Breathing (are they) • Circulation (pulses) • ECG (Is the monitor on?)
ASSESSMENT • What is the patients chief complaint? • Possible anaphylaxis? • If “NO” then assess treat & transport. • If ‘YES” get a Hx.
REVIEW • Chief Complaint • One or more symptoms for which the patient is seeking medical care • Most chief complaints are characterized by: • Pain • Abnormal function • A change in the patient's normal state • An unusual observation made by the patient (e.g., heart palpitations)
REVIEW • Chief Complaint • Be alert to the possibility that a chief complaint may be misleading or that a problem may be more serious than the patient's chief complaint • The patient • May not be exactly sure what is bothering him/her
If you suspect anaphylaxis then: Get a history of present illness (HPI). Be thorough, yet time efficient. ANAPHYLAXIS
REVIEW • History of Present Illness (HPI) • Identifies the chief complaint and provides a full, clear, chronological account of the symptoms • A thorough HPI requires skill in: • Asking appropriate questions related to the chief complaint • Interpreting the patient's response to those questions
Assess/obtain the patients vitals. Level of Consciousness Blood Pressure Pulse/ECG Respiratory rate Capillary refill SpO2 reading Skin ANAPHYLAXIS
ALLERGIES • Did you ask about allergies? • Did you look for a medical alert tag? • If unconscious, check for a medic alert tag.
ANAPHYLAXIS – S&S • Wheezing • Stridor • Hypotension (systolic less than 90) • Decreased LOC • Airway compromise • Edema • Urticaria ( with at least one of the above)
ANAPHYLAXIS ? • Does your exam identify: • Generalized urticaria? • Generalized or local edema?
TUNNEL VISION • Generalized urticaria!!! • How is the patients airway?
ANAPHYLAXIS - SOB • On exam do you note/observe any of the following? • Wheezing? • Stridor? • Shortness of breath?
ANAPHYLAXIS - SOB • If yes, then begin treatment. • Remember urticaria must be accompanied with wheezing and/or stridor, etc.
ANAPHYLAXIS - TREATMENT • Oxygen–NRB @ 15 L/min. • Epinephrine 1:1000 • If 30 kg give 0.3 mg • If 30 kg give 0.1 mg/10 kg rounding to nearest 0.05 mg.
WHY EPINEPHRINE? • Increases vascular smooth muscle tone (alpha agonist). • Decreases tone in alveolar smooth muscle (beta agonist).
ANAPHYLAXIS TREATMENT • Reassess patient • Be prepared to control their airway. • BVM • Suction
ANAPHYLAXIS TREATMENT • Repeat Epi x 1 if: • Condition does not improve after 10 minutes. • Patient deteriorates.
ANAPHYLAXIS TREATMENT • Remember OMITR • Oxygen • Monitor • Intervention(s) • Transport ASAP • Reassess often
SUMMARY • If patient has self-administered, follow the rules for a second administration • Following 1st Epi. If wheezing develops or is present consider the SOB protocol. • Urticaria alone is not an indicator for Epi.!