Download
1 / 28
280 likes | 433 Views
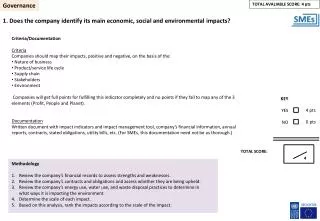
Chapter 8. HEALTHCARE GOVERNANCE. Alan Glasper and Rory Farrelly. This presentation examines the role of healthcare regulators in the UK. Focusing on the NMC, it illustrates the different functions a regulator fulfils.

E N D
Chapter 8 HEALTHCARE GOVERNANCE Alan Glasper and Rory Farrelly
This presentation examines the role of healthcare regulators in the UK. Focusing on the NMC, it illustrates the different functions a regulator fulfils. Use this presentation to stimulate discussion in your student learning group about the purpose of and need for a regulatory body in your area. Introduction
General Chiropractic Council General Dental Council General Medical Council General Optical Council General Osteopathic Council Nursing and Midwifery Council Pharmaceutical Society of NI Royal Pharmaceutical Society of GB UK Regulators of Healthcare Professionals
The Role of the Professional Regulator Sets Standards Regulator Approvescourses Keeps aRegister Takes action if necessary
The main purpose of the Nursing and Midwifery Council (NMC) in exercising its functions is to safeguard the health and well-being of persons using or needing the services of registrants. The NMC
ORIGINS OF THE NMC The battle for a professional, recordable qualification for nurses was protracted and hard. Florence Nightingale actually opposed registration. The fight for registration was led by Ethel Bedford Fenwick, the founder of The British Nurses Association.
THE FIGHT FOR REGISTRATION The Midwives Act passed in 1902 made the registration of general nurses an inevitability. A supplementary register of nurses included male nurses, mental nurses and fever nurses and, after a struggle, children’s nurses with learning disabilities following. It was many years, however, before registration of nurses enacted the creation of the General Nursing Council. The General Nursing Council (GNC) was the forerunner of today's NMC.
After a number of acrimonious amendments to the clauses of the Nurses Bill, Dr Christopher Addison, the Minister for Health, introduced his own Bill for the State Registration of Nurses. The Act was passed in December 1919.
GENERAL NURSING COUNCILS There were three General Nursing Councils (GNC): England & Wales, Scotland and Ireland. The Councils were established in 1921 with clearly prescribed duties and responsibilities for the training, examination and registration of nurses. The GNC was also responsible for approving training schools for the purpose of maintaining a Register of Nurses for England and Wales, Scotland and Ireland. The First Elections to the GNC on the 10th January 1923 General Nurses 10,887 Male Nurses 24 Mental Nurses 639 Sick Children’s Nurses 191 Fever Nurses 359 Total Eligible to Vote 12,097 Nurses
UKCC The GNC was replaced by the UK Central Council for Nursing, Midwifery and Health Visiting (UKCC), working in conjunction with four national boards which dealt with educational standards (1983-2001). Since 2001, the statutory body of nursing in the UK has been the Nursing & Midwifery Council (NMC) Sarah Thewlis is chief executive and registrar of the NMC.
The NMC was established under the Order and came into being on 1 April 2002, as the successor to the UKCC and the 4 National Boards. At that time the NMC adopted the existing rules and standards of the UKCC and where relevant, those of the National Boards. New rules for education, registration and registration appeals, midwifery and fitness to practise have since been developed. These came into force in August 2004
Key Responsibilities of the NMC • Maintain the register • Setting and improving standards • Giving advice • Dealing with misconduct and lack of competence • Quality assurance of education • Setting standards and improving guidance for midwifery supervision
The new register has 3 parts: Nurses (Part ONE) Midwives (Part TWO) Specialist Community Public Health Nurses (Part THREE) Maintaining the Register • Criteria for entry: • Proficiencies for each part of the register • Good health: to be able to practise safely and effectively • Good character: more than just absence of convictions – signing up to code of conduct • For the first time that the nurse registers, a second signature from another registrant will be required
Criteria for Maintenance on the Register • Fitness to Practise definition: • Good health and good character sufficient to practise safely and effectively • Adherence to the Code of professional conduct • Upholding public trust and confidence in the good reputation of the professions and the NMC
The NMC Code of professional conduct: standards for conduct, performance and ethics. The Code of Conduct outlines the duties of every nurse and midwife registered in the UK. It is intended to support safe and effective practice, and is an important tool in safeguarding the health and wellbeing of the public. Work is currently being undertaken on mental health standards of nursing to help nurses interpret the boundaries of professional performance and ethics within the context of the Code of Professional Conduct: standards for conduct, performance and ethics. Setting standards
The Professional Advisory Service is dedicated to providing nurses, midwives, specialist community public health nurses with free and confidential professional advice on the Council's standards. Advice can also be given to members of the public and other health service personnel Giving Advice
Old remit allegations: Misconduct Lack of fitness to practise due to ill health New remit allegations: Impairment of fitness to practise due to: Misconduct Lack of competence Conviction or caution for criminal offence Physical or mental health Fitness to practise deemed impaired by other regulatory body Incorrect or fraudulent entry in register Dealing with Misconduct and Lack of Competence
Previous sanctions: Interim suspension Removal – undefined period Caution for 5 years New sanctions: Interim suspension Interim conditions of practice Removal for at least 5 years Caution for 1-5 years Suspension from register Conditions of practice
Regulatory Failure Harold Shipman was convicted of 15 murders but is thought to have killed 236 patients
Between February and April of 1991 there were 26 unforeseen failures of medical treatment and unaccountable injuries on Ward 4 of Grantham and Kesteven General Hospital. In total four children died and nine were injured. Investigations found that enrolled nurse Beverley Allitt had altered critical settings on life support equipment and administered lethal doses of potassium and insulin to children in her care (The Allitt Inquiry, 1991). Nurse serial killer Beverly Allitt, who was given 13 life sentences for murdering and attacking children in her care has applied for a review of her sentence.
Fabricated and induced illness is rare but regulators must play their part in safeguarding children and adults in whom illness is fabricated or induced DoH guidance: http://www.dh.gov.uk/en/Consultations/Responsestoconsultations/DH_4017163 Allitt was described as having Munchausen syndrome by proxy but this is a term we no longer use
There is a Performance and Ethics Team which sits within the Directorate of Standards and Registration: Performance and Ethics Team: Susan Aitkenhead: Children’s Nursing John Mercy: Adult Nursing Joe Nicols (Head of Team): Mental Health and Learning Disabilities Rick Tucker: Mental Health and Prison Nursing Liz Plastow: SCPHN The P&E Team addresses: Medicines Management Code of Professional Conduct: standards for conduct, performance and ethics Record Keeping Standard Setting
Why is this important ? Role of HLSP (Higher Level Skills Pathfinder) New standards for mentors Quality Assurance of Education The Face of HLSP….. Q. What does he do?
HLSP has been appointed by the Nursing and Midwifery Council to ensure that nursing and midwifery education meets a consistently high standard across England, Scotland and Northern Ireland. • HLSPs: • Are a combination of educationalists and practitioners • Arrange their visits in advance • Decide that provision either meets or fails to meet requirements • When requirements aren’t met, an action plan is implemented to restore the provision
The NMC also: Keeps a live register of midwives Sets standards for practice, education and supervision of midwives Considers allegations of misconduct, lack of competence or unfitness to practise due to ill health Setting Standards and Improving Guidance for Midwifery Supervision
Other work by the NMC includes: Holding roadshows Running Code seminars Pre-registration work Post-registration work