Download
1 / 219
2.5k likes | 3.76k Views
Non alcoholic fatty liver disease (NAFLD) Diagnosis and evaluation. Raika Jamali M.D. Gastroenterologist and hepatologist Tehran University of Medical Sciences. Epidemiology.

E N D
Non alcoholic fatty liver disease(NAFLD)Diagnosis and evaluation RaikaJamali M.D. Gastroenterologist and hepatologist Tehran University of Medical Sciences
Epidemiology • NAFLD is one of the most common liver disorders in industrialized countries, with type 2 diabetes, obesity, hyperlipidemia, and cardiovascular disease being the most frequently evaluated and cited risk factors for the presence of NAFLD and accelerated disease.
The prevalence of NAFLD has been increasing along with the rise in obesity since the term non-alcoholic steatohepatitis (NASH) was coined by Ludwig in 1980. • Patients with NASH are more likely to have the metabolic syndrome than are those with mere steatosis.
The estimated prevalence in the general population depends on the type of screening test and ranges from 2.8% to 46% in unselected populations worldwide. • Ethnic variation in the prevalence of NAFLD/NASH has been described; several studies have indicated less common prevalence in African Americans.
Risk Score Model for Predicting Sonographic Non-alcoholic Fatty Liver Disease in Children and Adolescents • Cross-sectional study was conducted among 962 participants aged 6-18 years in Isfahan, Iran. • The sonographic findings of 16.8% of participants were compatible with NAFLD. Age, sex, body mass index, waist circumference and serum triglycerides level were diagnosed as factors associated with NAFLD. Hosseini SM, et al. Risk Score Model for Predicting Sonographic Non-alcoholic Fatty Liver Disease in Children and Adolescents. Iran J Pediatr. 2011 21(2):181-7.
In an autopsy study performed on 896 postmortem subjects at the Forensic Medicine Center in Tehran who died of acute incidents not related to hepatic disorders, 2.1% of cases were found to have NASH upon histological evaluation. Sotoudehmanesh R,, et al. Silent liver diseases in autopsies from forensic medicine of Tehran. Arch Iran Med. 2006 Oct;9(4):324-8.
Non-alcoholic fatty liver disease prevalence among school-aged children and adolescents in Iran • 966 children aged 7–18 years in Iran by a cross-sectional survey in 2007. • Fatty liver was diagnosed by ultrasound in 7.1% of children. The prevalence of elevated alanine aminotransferase (ALT) was 1.8%. NAFLD was significantly more common in the older group. Alavian SM, et al. . Non-alcoholic fatty liver disease prevalence among school-aged children and adolescents in Iran and its association with biochemical and anthropometric measures. Liver Int. 2009 Feb;29(2):159-63.
A recent review by Tilg and Moschen proposed the 'multiple parallel hits' hypothesis, where inflammation arises as a consequence of many parallel hits originating from visceral adipose tissue and/or gut; according to this hypothesis, gut-derived bacterial byproducts, cytokine and adipokine signaling, endoplasmic reticulum (ER) stress and innate immunity emerge as key factors in NASH pathogenesis.
KCs • KCs represent the largest group of tissue resident macrophages in the body. • They are able to release pro-inflammatory cytokines such as IL-1, IL-6, and TNFɑ which promote the infiltration of neutrophilic granulocytes to eliminate bacteria.
KCs also produce IL-12 and IL-18 which activate NK cells to produce anti-viral IFN γ. • However, following initial activation to produce pro-inflammatory cytokines, KCs releaseIL-10which down-regulates the production of TNFɑ, IL-6 and other cytokines and thereby probably contributes to the intrahepatic cell populations capability to induce tolerance.
Hepatic stellate cells • HSCs, well described for their participation in hepatic fibrosis and storage of vitamin A, have been shown recently to also function as APCs . • They are able to present lipid antigens to CD1d-restricted T cells, i.e. to NKT cells. • They are able to present protein antigens to conventional CD4+ or CD8+ T cells
Indeed, CD4 T cells can be converted to induced regulatory T cells (iTregs) by vitamin A derived retinoic acid and/or TGFβ . • Moreover, activated HSCs express the negative co-stimulator PD-L1 .
NAFLD pathogenesis in ob/ob mice Leptin deficiency Kupffer cellinhibited activation of dysfunction Hepatic stellate cells Hepatic NKT Increased adipokines cell depletion (resistin,adiponectin) inhibited liver fibrosis Th-1 polarization Despite Liver injury increased ROS Hepatocyte oxidative stress
Currently, it is widely accepted that lipopolysaccharide (LPS), a gut bacteria-derived endotoxin, is important for the development and progression of ASH and NASH through TLR-4 activation and induction of Kupffer cell activity.
Oxidative stress may directly activate an immune response and, subsequently, drive further inflammation, or may be the result of inflammation. • Hepatic oxidative stress, lipid peroxidation and ER stress can directly activate the inhibitor of NF-κB kinase or JNK to activate transcription of proinflammatory cytokines.
The best examples of pattern-recognition receptors include a group of Toll-like receptors (TLRs), which recognizes pathogen-associated molecular patterns to determine the presence of pathogens.
Once pathogens are identified, TLRs then induce multiple signaling pathways that regulate the expression of proinflammatory cytokines and chemokines to mount protective responses against invading pathogens.
Experimental and clinical data have demonstrated that levels of circulating and hepatic LPS are elevated in both ASH and NASH. • Increased LPS levels in NASH are likely owing to small intestinal bacterial overgrowth and alterations of the intestinal barrier.
Reportedly, Szabo’s group has determined that TLR-2, which recognizes lipoproteins and peptidoglycans from gram-positive bacteria, plays a protective role in NASH, but has no role in the pathogenesis of ASH.
Natural killer (NK) T cells are regulatory T lymphocytes that are preactivatedin situ by endogenous glycolipids, and are therefore considered to be innate immune effectors. • NKT cells are present in normal liver and are relatively depleted in steatosis. • Initial evidence points towards their fourfold increase in NASH-related cirrhosis, but there are no data on their numbers in early-stage NASH.
The adaptive immune response in NAFLD involves CD4+ T-helper cells, and although NASH is not classically considered a Th1-polarized disease, recent data suggest that its pathogenesis may be influenced by an imbalance between a relative excess of proinflammatory Th1 cytokines (i.e., IFN-γ) and a deficiency in anti-inflammatory IL-4 and IL-10 cytokines.
Emerging evidence also points towards a functional role of Th17-mediated T-cell responses in the pathogenesis of NASH. • Th17 cells are a recently described subset of CD4+ T-helper cells producing the cytokine IL-17. IL-17 can induce the expression of neutrophil-attracting chemokines in epithelial and endothelial cells, but it can also by itself mobilize and activate neutrophils. • In fatty liver, the characteristic perivenular infiltration of both neutrophils and lymphocytes suggests enhanced recruitment via their two major receptors CXCR1 and CXCR2.
Circulating, as well as liver and adipose tissue levels of TNF-α, are increased in animal models of obesity. • This is also true in humans, where TNF-α levels correlate with the degree of insulin resistance. • Furthermore, in humans, acute infusion of TNF-α inhibits insulin-stimulated glucose disposal,andcertain TNF-α polymorphisms are associated with susceptibility to insulin resistance and NAFLD,supporting the importance of this cytokine in the interaction among inflammation, insulin signaling, and fat accumulation.
Key points • Serum levels of TNF-α correlate with NASH activity however, levels of IL-6 do not. • Low serum levels of adiponectin have been strongly correlated with NASH.
The use of pentoxifylline, a known TNF-α inhibitor, has revealed mixed results. • In a small, open-labeled pilot study evaluating the use of pentoxifylline (1,600 mg/day) in patients with biopsy-proven NASH, improvement was documented in serum transaminase levels over a 12-month period.
In 2007, Satapathy et al. reassessed the use of pentoxifylline in patients with NASH, but at a dose of 1,200 mg/day over 12 months. • At the end of the study, serum transaminases and liver histology (including signs of liver injury, inflammation, and fibrosis) were significantly improved.[64]
Pentoxifylline is a relatively weak and nonspecific TNF-α inhibitor, and thus the use of more selective TNF-α blockers, such as infliximab and adalimumab, could potentially be more effective in the treatment of NAFLD. • Inhibitors targeted at IL-6 may be another potential target for preventing progression of steatohepatitis. • A humanized IL-6 receptor antibody, tocilizumab, has been developed to inhibit IL-6 binding to its receptor.
Tocilizumab has been investigated in clinical trials as a treatment for rheumatoid arthritis. • In a multicenter, randomized controlled trial in which patients were treated with tocilizumab or placebo over 3 months, tocilizumab significantly reduced disease activity in rheumatoid arthritis patients.[65, 66] • It is possible that this drug could be efficacious in NAFLD as well.
In addition, as it has been established that hypoadiponectemia is associated with disease progression, administration of adiponectin could potentially prevent development of severe steatohepatitis in patients with documented steatosis and mild steatohepatitis. • No human studies of adiponectin therapy have been performed to date.
As our understanding of the pathophysiology of NASH evolves, therapeutic targets for the treatment of NASH emerge. • One such potential target is NF-κBSelective targeting of NF-κB signaling of inflammatory cells may be crucial in therapy design, as NF-κB may also act as a hepatocellular survival factor, and its inhibition may therefore lead to enhanced apoptosis and compensatory hepatocyte proliferation, favoring HCC development.
A second selective target for NASH may be modulation of the JNK pathway. Selective blockade of JNK1 may be associated with improved hepatic steatosis, insulin resistance and inflammation; however, blockade of JNK2 may exacerbate hepatocellular injury. • Alternately, modulation of the gut flora or inflammatory cytokines may prove beneficial;[79] however, this has not been reproduced in human studies. Further work is needed to evaluate these and other potential therapeutic targets for NASH.
Signs and symptoms • Asymptomatic in majority of cases • Fatigue (not correlated with liver injury severity) • RUQ pain or discomfort • Hepatomegaly (50%) • Cirrhosis and portal hypertension • Obesity • Hypertension • Cardiovascular or cerebrovascular diseases • PCOD • OSA • Lipodystrophy (in non obese)
Diagnosis • NAFLD is a diagnosis of exclusion -Alcoholic Hepatitis -Drug induced Hepatitis (tamoxifen, amiodarone) -Viral Hepatitis -Autoimmune Hepatitis -Metabolic (Wilson and Hemochromatosis)
The most challenging DDX is alcoholic hepatitis • The histologic picture of both conditions is similar • Consumption of alcohol less than 10 g/d in women and 20 g/d in men
NAFLD is considered the hepatic manifestation of insulin resistance (metabolic) syndrome • Might be discovered incidentally in a check up • laboratory investigations alone have limitations for the diagnosis of NAFLD • Combination of imaging studies is necessary for the estimation of liver steatosis
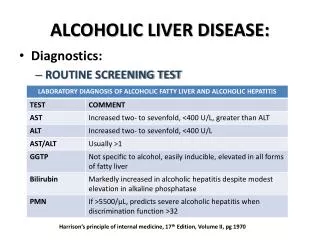
Laboratory Investigations • ~ 80% in normal range • None of the currently used tests are specific for the diagnosis of NAFLD • Aminotransferase elevation (< 4 times ULN) • It does not correlate with the severity of steatosis or fibrosis
AST/ALT ratio (AAR) > 1 suggesting cirrhosis • Higher AST , ALT levels and AAR are associated with NASH • The pattern of aminotrasferase elevation do not provide a distinction between simple fatty liver and NASH.
The differentiation between these conditions can be made by a histological approach. • The amount of liver fat can not be assessed using liver function tests • The degree of fat infiltration might be diagnosed using a variety of imaging modalities
Hyperbilirubinemia, hypoalbominemia and abnormal prothrombin time are present in cirrhosis • Hyperglycemia, hypertriglyceridemia, hypercholestrolemia are related to metabolic syndrome • HOMA (FIL X FPG / 22.5) is an estimate of insulin resistance • A correlation between HOMA and hepatic steatosis is demonstrated • Decreased apolipoprotein B is a rare cause of familial NAFLD (with normal LDL and HDL)
Serum Ferritin elevation (20-50%) • Indicates liver fibrosis not iron overload • Increased transferrin saturation (5-10%) • Hyperuricemia is associated with cirrhosis related deaths or hospitalizations • Alkaline phosphatase and GGT might be increased in advanced disease and might indicate the increased mortality • Autoantibodies might be present at low titers especially in advanced disease