Medication Management During Ramadan
370 likes | 586 Views
Understand Ramadan impact on medication management, psychological, & physiological health. Learn pharmacist opportunities & patient cases for cultural sensitivity training.

Medication Management During Ramadan
E N D
Presentation Transcript
Medication Management During Ramadan Cultural Sensitivity Training for Pharmacists
Outline • What is Ramadan? • Physiological/Psychological Impact • Medication management • Pharmacist Opportunities • Patient Cases
What is Ramadan? • A month of total abstention food, fluid, smoking, sexual activityfrom sunrise to sunset
What is Ramadan? • Occurs in the 9th month of the lunar Islamic calendar, for 28-30 days • Islamic calendar is 354 days, thus it precedes every year by 10-11 days
Why do Muslims Fast? • Self-discipline • Self-restraint • Exert control of the mind • Understand the plight of the less privileged and appreciate what one has • Increase good deeds, God-consciousness and purify the body and soul • Feelings of anger nullify the benefit of fasting • Attain spiritual peace
Upon reaching puberty, all healthy Muslims are required to partake in the fast
Exemptions • Children • Elderly • Chronically ill • Traveling* • Acutely ill* • Pregnant* • Breast-feeding* • Menstruating* • *temporarily exempt and can be made up at a later date Many Muslims who are eligible for exemption choose to fast nonetheless
Physiological Impact • No consistent data on the effect on lipid profiles • No significant changes in blood pressure or heart rate • Possible reduction in oxidative stress • Possible increase in gastric acidity • Weight gain/loss is largely dependent on night-time diet
Psychological Impact • Decrease in alertness • Increase in lethargy and irritability • Cognitive function decline • Alterations in normal circadian rhythms, with individuals becoming more active through the evening and at night, and sleep deprivation • Effects of tobacco, caffeine and energy and fluid intake
Life Adjustment • First meal (large) at sunset (Iftar) • Second (lighter) meal before dawn (Suhur) • 2013: July 9th – August 7th • 9:00 PM – 4:00 AM • ~ 7 hours of eating time/day • Single daily dose – morning or evening • 2 or more doses
Medication Management • Individualize therapy • Pay attention to drugs with a narrow therapeutic index • Switch to long-acting medications • Pay attention to Drug-Drug Interactions and Drug-Food interactions • Encourage extra monitoring • PLAN AHEAD!
Pre-Ramadan Medical Assessment • 1-2 months before Ramadan • Order blood work, examine glycemic control, blood pressure and lipids • Offer specific medical advice • Changes in diet or medication can be made early, so the patient can initiate fasting on a stable and effective program
Pharmacist Role • Encourage maintenance of a healthy diet • Encourage weaning off of caffeine and nicotine to avoid withdrawal symptoms • Opportunities! Quit smoking? • Discourage fasting during chronic illness, pregnancy and lactation
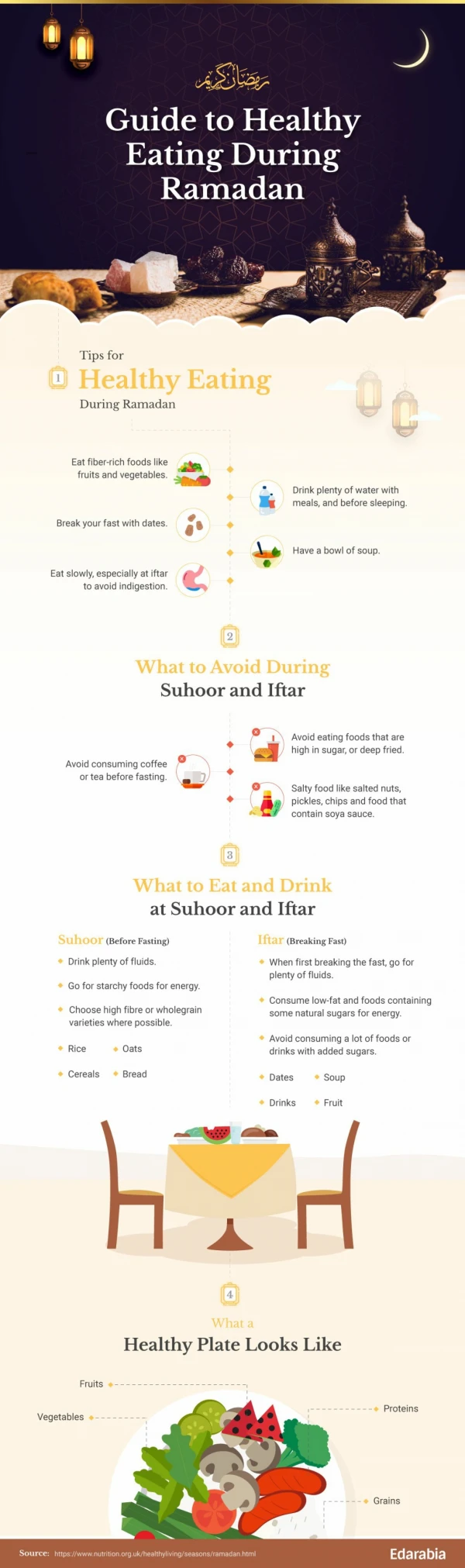
Dietary Advice • Continue to choose healthy foods • Don’t reward yourself! Eat healthy! • Remain hydrated during evening hours • Don’t skip suhur (morning meal) • Consume slow digesting foods (complex carbohydrates) and high protein foods • Don’t overeat. Don’t overindulge.
For more information… Ramadanmanagement.weebly.com
Patient #1 • Type II Diabetes, controlled, A1c = 7.5 • Hypertension • Hyperlipidemia Current Medication • Lantus (Glargine) long acting insulin 33 units ~ 6 pm daily • Metformin 2 500 mg tabs bid • Trandalapril 4 mg • Rosuvastatin 20 mg • Lifestyle: Moderate physical activity, bike-riding and jogging 3-4x per week • How would you change his insulin?
Patient #1 New Regimen: • Morning (before dawn) take 2 metformin 500 mg • Evening (break-fast) 9 pm, take all other oral medications, 2 metformin • Reduce long-acting insulin to 16 units at sunset meal • Add 8 units of Novo-rapid (Aspart) at sunset meal • Continue exercise– start light, increase workout later • Rationale: Would rather be on higher end than lower. • “By the time I master it, Ramadan is over”
Diabetes • EPIDIAR study is the largest collection of data on type I and type II diabetic patients that fast • 43% of patients with Type I Diabetes and 78% with Type II fasted for at least 15 days • Overall, the number of severe hypoglycemic episodes per month per patient were significantly higher during Ramadan compared to the preceding year (4.7 fold, 7.5 fold increased risk) • Increased risk of hyperglycemia associated with a change in diet
Insulin Management Type II: Maintain basal insulin to prevent fasting hyperglycemia. Use intermediate- or long-acting insulin preparations plus a short-acting insulin administered before meals Type I: Once or twice daily injections of intermediate or long-acting insulin along with premeal rapid-acting insulin
Patient #2 • 32 year old female patient • Gabapentin 300 mg TID for epilepsy partial seizures • Acetaminophen for headaches You advise Patient #2 not to partake in fasting. While she appreciates your advice, she says her religion is more important and she’s going to do it anyways. What do you do?
Patient #2 • Be respectful • Outline the risks clearly • Offer other alternatives (donating meals, charity, prayer) • Recommend she speaks with her religious guide (Imam)
Seizure frequency • Gomceli et al studied seizure frequency in Ramadan • Out of 114 patients, 38 had seizures and one of these developed status epilepticus • Statistically significant increase in frequency compared to months prior to Ramadan • Even patients on monotherapy, who did not change drug regimens, had an increase in seizure frequency
Offer Respect • Some patients may refuse your advice and continue fasting against medical wishes • Present the risks respectfully and understand that their spiritual reasoning may be different from yours • Fasting is a spiritual issue for which patients make their own decision after receiving advice from religious teachings and from health care providers • Our role is to provide information and let them decide
References • Leiper JB, Molla AM, Molla AM. Effects on health of fluid restriction during fasting in Ramadan. Eu J Clin Nutrition 2003 57 31-38 • AslamM, Healy MA. Compliance and drug therapy in fasting Moslem patients. J ClinHosp Pharm 1986;11:321-5. • Aadil B, Houti IE, Moussamih S. Drug intake during Ramadan. BMJ Volume 329. 2004. 778-782. • Trepanowski JF, Canale RE, Marshall KE et al. Impact of caloric and dietary restriction regimens on markers of health and longevity in humans and animals: a summary of available findings. Nutrition Journal 2011, 10: 107 • Recommendations for Management of Diabetes During Ramadan. Diabetes Care. 2010 33(8): 1895-1902 • EtemadyfarM. Effect of Ramadan on frequency of seizures. Abstract book, Congress on Health and Ramadan, October 2001. Tehran: Iranian Journal of Endocrinology and Metabolism, 2001: 32. • Mafauzy M, Mohammed WB, Anum MY et al. A study of the fasting diabetic patients during the month of Ramdan. Med J Malaysia 1990; 45: 14-7. • Dikensoy E, Balat O, Cebesoy B et al. The effect of Ramadan fasting on maternal serum lipids, cortisol levels and fetal development. Arch GynecolObset 2009; 279: 119-23. • Salti I, Benard E, Detournay B, et al. EPIDIAR study group. A population-based Study of Diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001(EPIDIAR) study. Diabetes Care 2004;27:2306-11.