Download
1 / 1
10 likes | 162 Views
Role of Antiretroviral Therapy, Viral Replication, and HIV Infection in Atherosclerosis. Priscilla Y. Hsue, Peter W. Hunt, Jeffrey N. Martin, Amanda Schnell, S. Craig Kalapus, and Steven G. Deeks

E N D
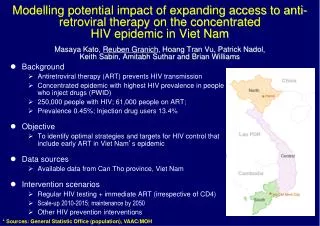
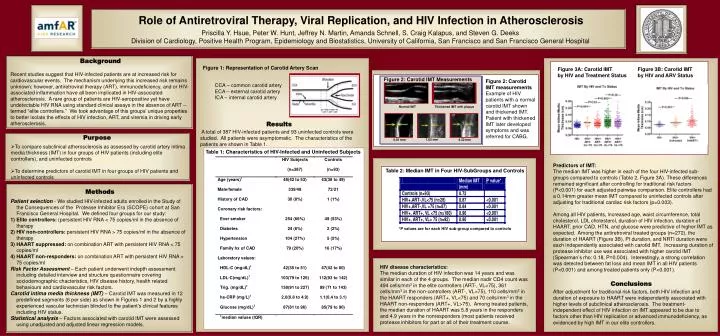
Role of Antiretroviral Therapy, Viral Replication, and HIV Infection in Atherosclerosis Priscilla Y. Hsue, Peter W. Hunt, Jeffrey N. Martin, Amanda Schnell, S. Craig Kalapus, and Steven G. Deeks Division of Cardiology, Positive Health Program, Epidemiology and Biostatistics, University of California, San Francisco and San Francisco General Hospital Purpose Table 1: Characteristics of HIV-Infected and Uninfected Subjects Background Figure 1: Representation of Carotid Artery Scan Figure 3A: Carotid IMT by HIV and Treatment Status Figure 3B: Carotid IMT by HIV and ARV Status Recent studies suggest that HIV-infected patients are at increased risk for cardiovascular events. The mechanism underlying this increased risk remains unknown; however, antiretroviral therapy (ART), immunodeficiency, and or HIV-associated inflammation have all been implicated in HIV-associated atherosclerosis. A rare group of patients are HIV-seropositive yet have undetectable HIV RNA using standard clinical assays in the absence of ART -- termed “elite controllers.” We took advantage of this groups’ unique properties to better isolate the effects of HIV infection, ART, and viremia in driving early atherosclerosis. Figure 2: Carotid IMT Measurements Figure 2: Carotid IMT measurements Example of HIV patients with a normal carotid IMT shown and thickened IMT. Patient with thickened IMT later developed symptoms and was referred for CABG. CCA – common carotid artery ECA – external carotid artery ICA – internal carotid artery Normal IMT Thickened IMT with plaque Results A total of 387 HIV-infected patients and 93 uninfected controls were studied. All patients were asymptomatic. The characteristics of the patients are shown in Table 1. 1.63 mm 0.81 mm 4.32 mm • To compare subclinical atherosclerosis as assessed by carotid artery intima media thickness (IMT) in four groups of HIV patients (including elite controllers), and uninfected controls • To determine predictors of carotid IMT in four groups of HIV patients and uninfected controls Predictors of IMT: The median IMT was higher in each of the four HIV-infected sub-groups compared to controls (Table 2, Figure 3A). These differences remained significant after controlling for traditional risk factors (P<0.001) for each adjusted pairwise comparison. Elite controllers had a 0.14mm greater mean IMT compared to uninfected controls after adjusting for traditional cardiac risk factors (p=0.003). Among all HIV patients, increased age, waist circumference, total cholesterol, LDL cholesterol, duration of HIV infection, duration of HAART, prior CAD, HTN, and glucose were predictive of higher IMT as expected. Among the antiretroviral treated groups (n=272), the duration of HAART (Figure 3B), PI duration, and NRTI duration were each independently associated with carotid IMT. Increasing duration of protease inhibitor use was associated with higher carotid IMT (Spearman’s rho: 0.18, P=0.004). Interestingly, a strong correlation was detected between fat loss and mean IMT in all HIV patients (P<0.001) and among treated patients only (P<0.001). Table 2: Median IMT in Four HIV-SubGroups and Controls Methods Figure 1 . Serologic Testing for HHV-8 • Patient selection - We studied HIV-infected adults enrolled in the Study of the Consequences of the Protease Inhibitor Era (SCOPE) cohort at San Francisco General Hospital. We defined four groups for our study: • Elite controllers: (persistent HIV RNA < 75 copies/ml in the absence of therapy • HIV non-controllers: persistent HIV RNA > 75 copies/ml in the absence of therapy • HAART suppressed: on combination ART with persistent HIV RNA < 75 copies/ml • HAART non-responders: on combination ART with persistent HIV RNA > 75 copies/ml • Risk Factor Assessment – Each patient underwent indepth assessment including detailed interview and structure questionnaire covering sociodemographic chacteristics, HIV disease history, health related behaviours and cardiovascular risk factors. • Carotid intima media thickness (IMT) – Carotid IMT was measured in 12 predefined segments (6 per side) as shown in Figures 1 and 2 by a highly experienced vascular technician blinded to the patient’s clinical features including HIV status. • Statistical analysis – Factors associated with carotid IMT were assessed using unadjusted and adjusted linear regression models. *P values are for each HIV sub-group compared to controls HIV disease characteristics: The median duration of HIV infection was 14 years and was similar in each of the 4 groups. The median nadir CD4 count was 494 cells/mm3 in the elite controllers (ART-, VL<75), 361 cells/mm3 in the non-controllers (ART-, VL>75), 110 cells/mm3 in the HAART responders (ART+, VL<75) and 70 cells/mm3 in the HAART non-responders (ART+, VL>75). Among treated patients, the median duration of HAART was 5.8 years in the responders and 4.9 years in the nonresponders (most patients received protease inhibitors for part or all of their treatment course. Conclusions After adjustment for traditional risk factors, both HIV infection and duration of exposure to HAART were independently associated with higher levels of subclinical atherosclerosis. The treatment-independent effect of HIV infection on IMT appeared to be due to factors other than HIV replication or advanced immunodeficiency, as evidenced by high IMT in our elite controllers.