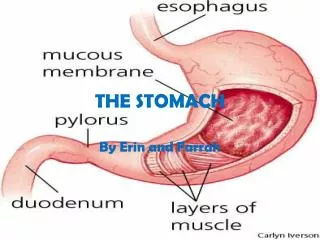
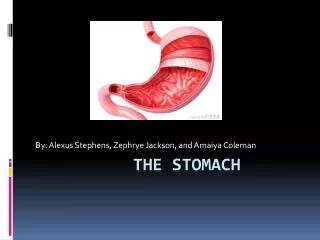
STOMACH
STOMACH. James Taclin C. Banez, MD, FPSGS, FPCS. Anatomy. Arterial blood supply Lymphatic drainage Nerve supply. PHYSIOLOGY. Function: Digestion of food, reduce the size of food Acts as reservoir Absorption of Vit. 12, iron and calcium Stimulant of Gastric secretion:


STOMACH
E N D
Presentation Transcript
STOMACH James Taclin C. Banez, MD, FPSGS, FPCS
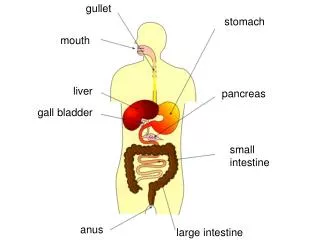
Anatomy • Arterial blood supply • Lymphatic drainage • Nerve supply
PHYSIOLOGY Function: • Digestion of food, reduce the size of food • Acts as reservoir • Absorption of Vit. 12, iron and calcium Stimulant of Gastric secretion: • Gastrin -----> (+) parietal cell • Acetylcholine (vagus) ---> (+) gastric cells • Histamine (mast cells) ---> parietal & chief cells
PHYSIOLOGY BAO: 2 – 5 meq of acid/hr. (vagal tone and basal histamine secretion) MAO: • Cephalic (vagus) ---> (+) parietal & G cell • 10 meq acid/hr. • Gastric: ---> (+) vagus & G cell • 15 – 25 meq of acid/hr pH = < 2.0 • Intestinal: • Chyme enters the duodenum • (-) gastric release • Secretin, gastric inhibitory peptide, peptide YY • ACID condition sterilized the area, except for HELICOBACTER PYLORI
GASTRIC DISEASES: • Acid peptic Disease • Neoplasm
Acid peptic Disease: • Due to imbalance in the normal interplay between acid-pepsin and mucosal defense mechanism • Types: • Acute Gastritis (erosive): • Inflammation confined in the mucosa • True Ulcers: • Extends through the mucosa
Peptic ulcer • Duodenal Ulcer • Gastric Ulcer Duodenal ulcer > gastric ulcer Female > Male Duodenal ulcer is younger by 10 yrs Location: • Duodenal: • duodenal bulb • Hyper-secretion of acid
Peptic ulcer Location: • Gastric Type I - proximal antrum and body (disturbance in mucosal defense) Type II - arises secondary to duodenal ulcer w/ pyloric stenosis Type III - Prepyloric and pyloric channel - (hyper-secretion of acid)
Peptic ulcer Pathogenesis: • For both Duodenal & Gastric Ulcers: • Infection w/ H. pylori: • Decreases resistance of mucus layer from acid permeation (hydrophobicity) • Increase acid secretion • Slow duodenal emptying • Reduced both duodenal and gastric bicarbonate secretion
Peptic ulcer Pathogenesis: • Effects of NSAIDs • Decreases Prostagladin Prostaglandin – inhibits acid secretion, stimulates mucus and HCO3 secretion and mucosal blood flow • Zollinger-Ellison Syndrome(1%): • Massive secretion of HCL due to ectopic gastrin production from non-beta islet cell tumor (gastrinoma) • Associated w/ type I (MEN) PPP • 20% multiple, 2/3 malignant, w/ slow growing • Parietal cell mass is increased • > gastrin 3-6 x the normal
Peptic ulcer • For Duodenal • Acid Hypersecretion: • More parietal and chief cells • Genetic • Due to release of tophic factors - gastrin • Increase capacity of individual cell to secret • Gastric Motility abnormality • Impaired duodenal acid disposal • Reduced basal and peak duodenal bicarbonate secretion and defect in mucus
Peptic ulcer • For Gastric Ulcer: • Reflux of Duodenal contents (pancreas and biliary) • Gastritis -----> Ulceration • Pyloric sphincter dysfunction • Cigarette smoking: • Increases duodeno-gastric reflux • Decrease prostaglandin synthesis • Decreases duodenal, gastric and pancreatic bicarbonate secretion • Bile acids, lysolecithin and pancreatic secretions – disturb surface mucus layer
Clinical Manifestation • Abdominal pain: • Due to irritation of afferent nerves w/in the ulcer by the acid or due to peristaltic waves passing through the ulcer • Duodenal: colicky or burning pain relieved w/ food intake • Gastric: gnawing or burning usually during or after eating. • N/V • Weight loss • Epigastric tenderness
Diagnosis: • UGIS (double contrast) • Endoscopy
Treatment: • Medical: Avoid the following: • Smoking • Aspirin / NSAIDs • Coffee (acid secretion) • Alcohol (damage the mucosa) Mechanism of Pharmacologic Therapy: • Neutralize gastric secretion (HCL): ANTACID • Inhibits Secretion of Acid: • H2 receptor antagonist – CIMETIDINE, RANITIDINE, FAMOTIDINE
Treatment: Mechanism of Pharmacologic Therapy: • Inhibits Secretion of Acid: • Anticholinergic: • Inhibits acetylcholine Pirenzepine HCL • H+ / K+ - ATPase inhibitor proton pump • Benzimidazole selectively inhibits parietal cells Omeprazole, Lanzoprazole, Pantoprazole • Protection of Gastric Mucosa: • Prostaglandin: Methylated E2 analog inhibits gastric secretion, increases mucosal bld flow & HCO3 & mucosa secretion
Treatment: Mechanism of Pharmacologic Therapy: • Protection of Gastric Mucosa: • Sulfated disaccharide (sucralfate) • Binds to protein in the ulcer as protective coat • It can inhibits peptic activity • Colloid bismuth • Binds w/ protein & against H. pylori
Treatment: Mechanism of Pharmacologic Therapy: • For eradication of H. pylori: • Bismuth based triple therapy • Bismuth + Tetracycline + Metronidazole • Proton pump inhibitor • Omeprazole + Amoxicillin/Clarithromycin + metronidazole
Treatment: Surgical Treatment: Indication: • Intractability: • Highly selective vagotomy • Low septic complication, (-) dumping and diarrhea • For gastric ulcer: • Total or subtotal gastrectomy w/ or w/o vagotomy
Treatment: Surgical Treatment: Indication: • Hemorrhage: s/sx • Critically ill • Endoscopy • Surgery: a. continue bleeding for more than 6 units b. recurrent bleeding after endoscopically controlled - pyloroduodenostomy + HSV - pyloroduodenostomy + vagotomy + pyloroplasty
Treatment: Surgical Treatment: Indication: • Perforation: S/Sx • Graham omental patch only for shock, perforation > 48 hrs or other medical problem • Vagotomy + pyloroplasty; HSV • Vagotomy + Gastrojejunostomy • Obstruction: S/Sx; Saline loading test • Vagotomy + Antrectomy • Vagotomy + Gastroenterostomy
Acute Gastritis (erosive) • Stress erosions are usually multiple, small punctuate lesion in the proximal acid secreting portion of the stomach Clinical Settings: • Severe illness, trauma, burns (Cushing ulcer) or sepsis • Due to (-) mucosal defense (ischemia) • Drug and Chemical ingestion • Aspirin / NSAIDs • CNS trauma: • Increase gastrin ---> elevated acid secretion • Curling ulcer
Acute Gastritis Pathogenesis: • Aspirin, bile salts (backflow), alcohol • Mucosal ischemia Clinical manifestations: • Gastrointestinal bleeding • Abdominal pain Diagnosis: • Endoscopy / radionuclide scanning / visceral angiography
Acute Gastritis Treatment: • NPO • NGT / Saline lavage • Antacids / omeprazole / sucralfate • Intra-arterial infusion of vasopressin • Surgery --> if 6-8 units over 24 hrs • Mortality ---> 40% • Near total gastrectomy • Vagotomy + pyloroplasty + over sewing of bleeder • Partial gastrectomy + vagotomy
Zollinger-Ellison Syndrome (Gastrinoma) • Symptoms tends to be more severe, unrelenting and less responsive to therapy. Clinical Manifestation: • Pain • Diarrhea • Steatorrhea Diagnosis: • Acid secreting studies (50meq/hr) • UGIS • Radio-immuno assay for serum Gastrin level • Diff: a) Pernicious anemia b) Renal insufficiency c) Antral gastrin hyperplasia or hyperfunction • CT scan and angiography to localize gastrinoma • Venous sampling
Gastric Neoplasm: • 90% malignant • 95% adenocarcinoma • 4% lymphoma • 1% leiomyosarcoma (GIST-malignant gastrointestinal stromal tumors) • Rare – carcinoid, angiosarcoma, squamous cell CA. • As metastatic lesion of --> - colon/pancreas - melanoma/breast • Malaysia, Chile, Iceland and JAPAN • Male:Female (2:1); more common twice in black than white • 6 -7 decade of life: if it occurs in young(30-40y/o) becomes more aggressive (linitis plastica or signet ring histology) • Low socioeconomic
Adenocarcinoma: Etiology: • Diet - high in nitrates----->nitrites (bacteria & bile salts) - pickled, salted or smoked food - fresh fruit & vegetable and vit C & E ---> lowers • H. pylori infection • 3 fold increase risk • Ebstein Barr virus • Genetic factor: • Suppression of p53 (tumor suppression gene); • over expression of COX-2
Adenocarcinoma: Etiology: • Cigarette smoking (alcohol (-) effect) • Gastric polyp: (epithelial, inflammatory, hamatomatous, heterotopic, hyperplastic & adenoma) – adenoma & hyperplastic polyps can lead to CA. • Chronic atrophic gastritis (CAG): • Most common precursor of CA (intestinal type) • H. pylori causes CAG
Adenocarcinoma: Etiology: • Intestinal metaplasia: (H. pylori) • Benign gastric ulcer: • It is now generally recognized that all gastric ulcers are cancer until proven otherwise • Previous Gastric resection: • 10 yrs later near the stoma • Others: - Radiation exposure - Family hx - Pernicious anemia - Bld type A (1.2 risk)
Pathology: Gastric dysplasia ---> precursor of gastric CA Early gastric cancer: Limited to the mucosa and submucosa, regardless of LN status 70% are well differentiated Cure rate is 90% Gastric Neoplasm:
Pathology: Macroscopic Subtypes: • Superficial spreading • Polypoid (well differentiated) • Fungating • Ulceration • Scirrhous (linitis plastica): infiltrates the entire thickness of the wall • Leather bottle stomach • Poor prognosis • Usually undifferentiated Location of primary tumor: • 40% distal / 30% middle / 30% distal
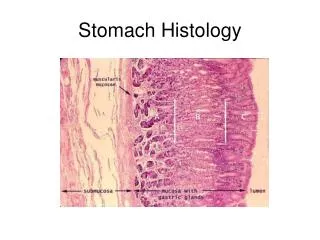
WHO Classification: Adenocarcinoma: Papillary adenocarcinoma Tubular adenocarcinoma Mucinous adenocarcinoma Signet-ring cell carcinoma Adenosquamous carcinoma Squamous cell CA Small cell CA Undifferentiated CA Others Lauren Classification: Intestinal type (53%) Diffuse type (33%) Unclassified (14%) Ming Classification: Expanding type (67%) Infiltrative type (33%) HISTOLOGY:
Microscopic Subtypes: • Intestinal Type • Diffuse Type:
Histologic type: • Papillary • Tubular • Mucinous • Signet ring Mode of spread: • Direct • Lymphatic • Hematologic • Transcoelomic route
Clinical Manifestation: • Weight loss due to anorexia and early satiety is the most common symptoms • Abdominal pain (not severe) common • Nausea / vomiting • Chronic occult blood loss is common; GIT bleeding (5%) • Dysphagia (cardia involvement)
Clinical Manifestation: • Paraneoplastic syndromes ( Trousseau’s syndrome – thrombophlebitis; acanthosis nigricans – hyperpigmentation of axilla and groin; peripheral neuropathy) • Signs of distant metastasis: • Hepatomegally / ascites • Krukenbergs tumor • Blummers shelf (drop metastasis) • Virchow’s node • Sister Joseph node (pathognomonic of advances dse)
Diagnosis: • UGIS (double contrast) • Endoscopy (Biopsy / Ultrasound) • GOLD STANDARD • Best pre-operative staging • Needle aspiration of LN w/ ultrasound guidance • Can even give preop neoadjuvant tx • CT scan (intravenous and oral contrast): • For pre-operative staging • Whole body Positron Emission Tomography scanning (PET): • Tumor cell preferentially accumulate positron-emitting 18F fluorodeoxyglucose.
TREATMENT: SURGERY: • The only curative tx for gastric cancer • Except: • Can’t tolerate abdominal surgery • Overwhelming metastasis • Palliation is poor w/ non-resective operations • GOAL: resect all tumors, w/ negative margins (5cm) and adequate lymphadenectomy (need for RFS) • Enbloc resection of adjacent organ is done if needed.
TREATMENT: SURGERY: Radical subtotal gastrectomy Standard operation for gastric cancer Organs resected: Distal 75% of stomach 2 cm of duodenum Greater & lesser omentum Ligation of R & L gastric artery and gastroepiploic vesels Billroth II gastojejunostomy
TREATMENT: SURGERY: Radical subtotal gastrectomy Standard operation for gastric cancer If gastric remnant left is small (<20%) do Roux-en-Y reconstruction
Extent of lymphadenectomy: N1 – 3 to 6 N2 – 1, 2, 7, 8 & 11 N3 – 9, 10 & 12 N1 nodes are w/in 3cm of the tumor N2 along hepatic & splenic arteries N3 more distant nodes Agreed upon: to avoid under staging of gastric CA, a minimum of 15 nodes should be resected w/ the gastrectomy specimen.
Adjuvant Treatment for Gastric Carcinoma: • Chemotherapy: • 5-fluorouracil, leucovorin, cisplatin, doxorubicin and methotrexate • Can not prolong survival in unresectable, metastatic or recurrent diseases • Radiation (4500cGy): • Effective in palliation for pain and bleeding • For stages II and III adenocarcinoma
Radical subtotal gastrectomy: • D1 resection (standard in USA): • Removes tumor and N1 • D2 resection(standard in Asia): • Gastrectomy and N1 and N2 removal • Removes the peritoneal layer over the pancreas and anterior mesocolon • Removes LN along hepatic & splenic • Splenectomy and distal pancreatectromy not routinely removed due to higher morbidity postop.
Endoscopic Resection of Gastric Carcinoma Criteria: • Tumor < 2cm in size • Node negative • Tumor confined on the mucosa Nodes metastasis is < 1%: • No mucosal ulceration • No lymphatic invasions • <3cm tumor
Screening of Gastric Cancer • Patients at risk for gastric CA should undergo yearly endoscopy and biopsy: • Familial adenomatous polyposis • Hereditary nonpolyposis colorectal cancer • Gastric adenomas • Menetrier’s disease • Intestinal metaplasia or dysplasia • Remote gastrectomy or gastrojejunostomy