Download
1 / 22
220 likes | 434 Views
PRIORITY MEDICINES FOR EUROPE AND THE WORLD . A report prepared by WHO for the Netherlands Government by Warren Kaplan Richard Laing and. Saloni Tanna Marjolein Willemen Eduardo Sabaté Monique Renevier Joyce Wilson Lisa Greenough Ann Wilberforce Kathy Hurst.

E N D
PRIORITY MEDICINES FOR EUROPE AND THE WORLD A report prepared by WHO for the Netherlands Government by Warren Kaplan Richard Laing and • Saloni Tanna Marjolein Willemen • Eduardo Sabaté Monique Renevier • Joyce Wilson Lisa Greenough • Ann Wilberforce Kathy Hurst
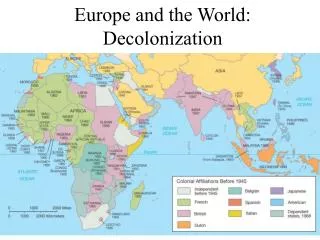
Objectives of Priority Medicines Project • Provide a methodology for identifying pharmaceutical “gaps” from a public health perspective, for Europe and the World . • Provide a public-health based pharmaceutical R&D agenda for use by the EU in the 7th Framework Programme, “Good public policy should spend public funds on areas of greatest public needs”
Special Needs for Women, Children, and the Elderly • All groups neglected in drug development • Complicated by different physiology & metabolism • Recent improvements in situation of women and children • Considerable gaps remain for the elderly who use the most medicines
Promoting Innovation and Removing Barriers • Public Private Partnerships may be a vehicle to address market failure • Pricing issues are critical to the future of the European pharmaceutical industry. Propose investigating differential pricing based on GNI per capita and efficacy measures. Reseach prospective price setting. • EMEA, FDA, Rawlins and Industry have all proposed similar measures to remove barriers • Comparative trials provide critical information on head to head comparisons. Use of European databases may facilitate such studies
Differential Pricing: Indicative prices in US$/annum of highly active antiretrovirals (HAART) and a new hypothetical regimen in countries of variable wealth
Barriers to Innovation: Background • Cost and duration of medicines development have increased • Many projects in early development stages, but not enough of this potential innovation is being translated into market approvals. • For some diseases, there remains an inadequate understanding of basic science, and potential targets for medicines development have not been identified.
Recent Publications • Four papers published almost simultaneously, plus commentary on Priority Medicines website • EMEA: Discussion Paper: The European Medicines Agency Road Map to 2010: Preparing the Ground for the Future • FDA: " Challenge and Opportunity on the Critical Path to New Medical Products" • Perspectives – "Cutting the Cost of Drug Development?" M.D. Rawlins • Sue Middleton: GSK Commentary on "Barriers to Innovation"
Barriers to Innovation:Suggested Solutions • All authors agreed that every aspect of the regulatory process should be re-examined and that the evidence base for regulatory practices should be critically analysed using modern methodologies. • Preclinical studies • Many old tests and methods • New analytic tools needed • Validation of old methods required • Clinical Studies • Regulatory authorities are risk averse so the RCT has become the gold standard • Other approaches even using historical controls may be possible and desirable
Neglected Areas:Post marketing Surveillance and Patients • All papers neglect Phase IV studies as a part of the innovation process. Great opportunities for Europe from use of electronic data bases for Phase IV studies on both efficacy and safety • Apart from the industry paper, none of the three other papers mention any role for patients in this review. They are referred to as beneficiaries of the process but never as contributors to the decision-making.
Role of Patients remains unclear • Patients have speeded innovation e.g. AIDS and Orphan diseases • Valuable role in treatment guideline development emerging e.g. NICE • Patients play important role in ethical & hospital committees e.g. IRB & DTCs • Will now be part of CSM in UK • Future role likely to be important and growing
A "barriers to innovation" Research Agenda • Bottlenecks and barriers in the current medicines development process are to be identified and solutions elaborated to overcome them. • Range of stakeholders required: academia, clinicians, patient organizations, large and small industry, regulatory and ethics specialists • Every requirement within the medicines development process whether clinical or preclinical should be questioned for its regulatory relevance, costing, and predictive value. • The involvement of the EMEA and the various European national regulatory agencies and their scientists is critical to this initiative. • 6th Framework already has issued a call closing November 16th
PRIORITY MEDICINES FOR EUROPE AND THE WORLD Comparative Clinical Trials Chapter 8.4 Warren Kaplan
Comparative Trials: Background • For most medications at launch, we know little about whether or not a given medication is better value for the money than alternatives. • This knowledge gap exists because most drug regulatory authorities do not examine "value for money" • For most medications at launch, clinical trials are not designed to look at whether or not a given medication is better than another drug. • Typically, efficacy is measured versus a control which is often, but not invariably, a placebo lacking any active ingredient. • Many registration authorities do require comparative benefit studies • To estimate comparative benefit between two medicines, large (time consuming and expensive) trials are needed since there are often small differences between treatment outcomes when comparing the interventions.
Comparative Trials: Who should pay for them and who conducts them? • Industry? Government? Or… • Private insurers and the government could set aside some fraction of their annual medicines spending to endow an organization to provide an independent source of reputable research into comparative effectiveness and cost. • Electronic prescription and medical databases to conduct Phase IV and/or pharmacoepidemiologic studies in place of controlled, comparative clinical trials. • EU has a great comparative advantage over the USA as this kind of electronic linkage of prescribers and medical records is still fragmented in the USA • Phase IV studies could add a randomization step ("randomized epidemiology")
Comparative Trials/Comparative Effectiveness • Europe 2005: "An information society for all", available at http://europa.eu.int/information_society/eeurope/2002/news_library/documents/eeurope2005/eeurope2005_en.pdf. • This Action plan on "electronic health" should be used as a way of creating post-marketing studies to better understand comparative effectiveness and cost-effectiveness.
General Conclusions • Commonality of interest exists for chronic diseases between Europe and the World • Priorities can be set based on evidence, trends and projections and social solidarity • Pharmaceutical gaps exist as a result of biological challenges and market failure • Highest priorities are antibacterial resistance, influenza, smoking and neglected diseases • Pricing issues and barriers to innovation strongly affect the European industry • The EU needs to find a way to support translational research for market failure pharmaceutical gaps
Regulatory Conclusions • Common view as to how regulatory obstacles serve as a barrier to innovation • Different solutions proposed by different stakeholders. All should be considered • Striking lack of attention to Phase 4 activities. Vioxx and FDA hearings may change everything • Strong interest in routine use of large (even complete) patient data bases • A researchable topic!
Priority Medicines Project For further questions, please contact: laingr@who.int wak22@comcast.net +41-22-791-4533 http://mednet3.who.int/prioritymeds/report/index.htm