Download
1 / 45
450 likes | 479 Views
Explore diagnostic grids and key questions on atrial fibrillation, ventricular tachycardia, and more with Dr. Susan P. Torrey. Learn to differentiate tachycardia types through EKG criteria. Discover insights on treatment options and challenges in emergency care.

E N D
Terrifying Tachycardias Susan P. Torrey, MD, FACEP, FAAEM Associate Professor of Emergency Medicine UMass Medical School – Baystate Medical Center Springfield, Mass
I have no disclosures TorreyEKG.com
Objectives • Consider the diagnostic grid • Answer several interesting questions • What’s the scariest atrial fib you’ll ever see? • How DO you know it is ventricular tach?
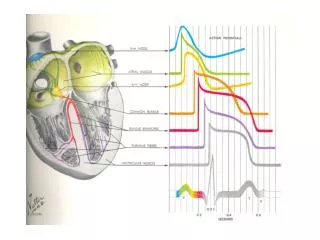
Rate Rate = 300 ÷ # “big boxes” between R-R 300 – 150 – 100 – 75 – 60 – 50
Diagnostic grid - tachycardias Cherchez le P
Sinus tachycardia • normal P before every QRS • upright P in lead II
Sinus tachycardia • Emergency Department differential: • compensation for shock - dehydration, hemorrhage, sepsis • fever • drugs (cocaine, anticholinergic) • acute pulmonary embolism • thyrotoxicosis • anxiety - only as a dx of exclusion
Atrial flutter • atrial activity – regular deflections (F waves) - F waves usually 300/minute • rate and regularity of QRS variable - in purest form, multiple of 300
Atrial flutter • untreated, flutter usually has 2:1 AV block regular rhythm at 150/minute
Rate of 150… • when the rate is 140 – 150/minute always consider 2:1 atrial flutter
Supraventricular tachycardia • Regular, narrow tachycardia due to re-entry • AV nodal re-entry vs. AV re-entry (WPW) • Onset and termination is abrupt • Heart rate 140-220/minute • Differential: sinus tach, 2:1 flutter, ? a fib
Atrial fibrillation • no discernible P waves - atrial activity is fibrillatory waves (f) - fibrillatory waves – II and V1 • ventricular rhythm is irregularly irregular - untreated ventricular rate 100 – 180/min
Multifocal atrial tachycardia • P waves of varying morphology (≥ 3 foci) - absence of single dominant P wave • Variable PP, RR, PR intervals - theother irregularly irregular rhythm • Seen with COPD, elderly, seriously ill
Diagnostic grid - tachycardias • aberrancy • pre-existing BBB • bypass tract
Ventricular tachycardia • Abnormal wide QRS • Regular rhythm – “dead regular” • Rate usually 140-200/minute
Diagnostic grid - tachycardias • aberrancy • pre-existing BBB • bypass tract
What is the scariest tachycardiayou will ever see? 38-year-old man with history of palpitations
Scary atrial fib • Atrial fib with… - aberrancy - pre-existing bundle, or… - bypass tract with Wolff-Parkinson-White! - changing QRS shape and rapid conduction
Atrial fib with WPW • most AV node blockers ↑ bypass conduction • must avoid A – B – C – D • A – adenosine • B – beta-blockers • C – calcium-channel blockers • D – digoxin • treat with electricity or procainamide
What about amiodarone? • 2005 ACLS – rec: amiodarone • 2010 ACLS – returns to procainamide Simonian S Inter Emerg Med 2010 • Literature review challenges superiority and safety of amiodarone for atrial fib with WPW • Complex drug with effects on Na+, K+, and Ca++ channels, as well as α- and β-blocking effects
rapid atrial fib with wide complex after cardioversion after ablation of bypass tract
How do you know if it’s V. tach? • EKG criteria favoring V. Tach • AV dissociation
How do you know if it’s V. tach? • EKG criteria favoring V. Tach • AV dissociation • QRS concordance • all chest leads (V1-6) predominantly negative
How do you know if it’s V. tach? • algorithms • Brugada’s four-step algorithm 98% sens / 96% spec • Circ 1991 • Vereckei’s new “simplified” algorithm • Euro Heart J 2007
How do you know if it’s V. tach? • clinical predictors • association with heart disease or MI 98% positive predictive value • Aktar Ann Intern Med 1988
In conclusion… • Remember, tachycardias are easy… • Narrow or wide complex? • Regular or irregular?
In conclusion… • Remember, tachycardias are easy… • Narrow or wide complex? • Regular or irregular? • If the rate is around 150 think 2:1 flutter.
In conclusion… • Remember, tachycardias are easy… • Narrow or wide complex? • Regular or irregular? • If the rate is around 150 think 2:1 flutter. • Rapid wide-complex atrial fib think WPW… • Avoid A – B – C – D
In conclusion… • Remember, tachycardias are easy… • Narrow or wide complex? • Regular or irregular? • If the rate is around 150 think 2:1 flutter. • Rapid wide-complex atrial fib think WPW… • Treat wide-complex tachycardia per ACLS