Download
1 / 49
490 likes | 492 Views
This article provides an overview of brown tumors and hyperparathyroidism, including their causes, symptoms, and treatment options. It also discusses the role of parathyroid hormone and its effects on calcium regulation in the body.

E N D
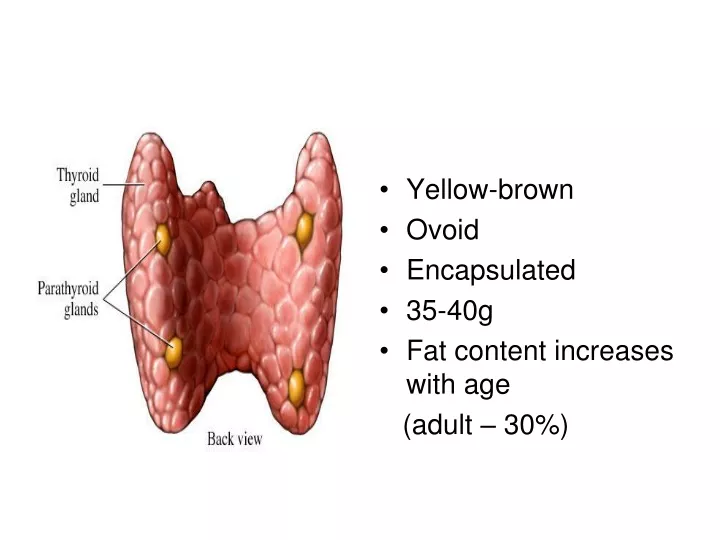
Yellow-brown • Ovoid • Encapsulated • 35-40g • Fat content increases with age (adult – 30%)
CHIEF CELLS polygonal central round nucleus light-dark pink cytoplasm some “water-clear” PARATHYROID HORMONE (PTH) • Oxyphil cells
Calcium • Muscle contraction, intracellular messenger systems, cardiac repolarization. • Exists in free and bound states Albumin Phosphate & Citrate • Concentration of Ca++ mediated by • Parathyroid gland • Parafollicular C cells • Kidney • Bone
Parathyroid Hormone • Bone • Kidney • GIT
Parathyroid Hormone • Stimulates renal conversion of 25-(OH)D3 to 1,25-(OH)2D which increases intestinal Ca++ absorption • Directly stimulates renal Ca++ absorption and PO43- excretion • Stimulates osteoclastic resorption of bone
Hyperparathyroidism • occurs in two major forms —primary- represents an autonomous, spontaneous overproduction of PTH - secondary - typically occur as secondary phenomena in individuals with chronic renal insufficiency —tertiary – from secondary
The frequency of the various parathyroid lesions underlying the hyperfunction is as follows: • Adenoma: 85% to 95% • Primary hyperplasia (diffuse or nodular): 5% to 10% • Parathyroid carcinoma:∼1%
Parathyroid adenomas • Solitary nodule • 0.5 to 5.0 gm; • well-circumscribed, • soft, • tan to reddish-brown • mostly composed chief cells
Technetium-99m radionuclide scan demonstrates an area of increased uptake corresponding to the left inferior parathyroid gland
Primary hyperplasia • classically all four glands are involved • sporadically or as a component of MEN syndrome • In contrast to primary hyperplasia, the glands outside the adenoma are usually normal in size or somewhat shrunken - feedback inhibition by high levels of serum calcium
Primary hyperparathyroidism may be: • asymptomatic - identified after a routine chemistry profile, or (2) associated with the classic clinical manifestations of primary hyperparathyroidism.
Renal • Nephrolithiasis – STONES! • Nephrocalcinosis - calcification of the interstitium & tubules
Gastrointestinal disturbances, - constipation, nausea, peptic ulcers, pancreatitis, gallstones - GROANS!
Neuromuscular abnormalities - weakness, fatigue. • CNS alterations - depression, lethargy, - MOANS! - seizures
Skeletal changes – BONES! • increased osteoclasts - erode bone matrix & mobilize calcium • Bone resorption is accompanied by increased osteoblastic activity • & the formation of new bony trabeculae with widely spaced, delicate trabeculae
Hyperparathyroidism with osteoclasts boring into the center of the trabeculum – railroad tracks
Skeletal changes In more severe cases • the cortex is grossly thinned, and the marrow contains increased amounts of fibrous tissue accompanied by foci of hemorrhage & cyst formation (osteitis fibrosa cystica)
Skeletal changes • Aggregates of osteoclasts, reactive giant cells, & hemorrhagic debris occasionally form masses that may be mistaken for neoplasms (brown tumours of hyperparathyroidism). differential diagnosis – bone tumours with giant cells
Hypercalcemia • relatively common complication of malignancy • solid tumors, - lung, breast, head & neck, renal cancers • multiple myeloma • osteolytic metastases. • many solid cancers secrete PTH-related protein (PTHrP)
Hypoparathyroidism • Surgically induced • Autoimmune • Congenital absence of parathyroid glands • Genetic abnormalities
Tetany • The hallmark of hypocalcemia - decreased concentration in serum of ionized calcium • neuromuscular irritability • circumoral numbness • paresthesias (tingling) of the distal extremities • carpopedal spasm • life-threatening laryngospasm • generalized seizures
Pseudohypoparathyroidism • hypoparathyroidism occurs because of end-organ resistance to the actions of PTH
1 cm, <0.5g • two morphologically & functionally distinct components: anterior lobe (adenohypophysis)– 3/4 posterior lobe (neurohypophysis)– 1/4.
Hypophyseal-Pituitary Axis • Site of Neural – Hormonal interaction • Sets temporal release of hormones
Anterior Pituitary cells • eosinophilic cytoplasm (acidophil), • basophilic cytoplasm (basophil), • poorly staining cytoplasm (chromophobe)
Five Cell types • 1. Somatotrophs, - growth hormone (GH) acidophilic - half of all • 2. Lactotrophs (mammotrophs) acidophilic - prolactin (lactation) • 3. Corticotrophs: basophilic adrenocorticotropic hormone (ACTH), pro-opiomelanocortin (POMC), melanocyte-stimulating hormone (MSH), endorphins, lipotropin.
4.Thyrotrophs: basophilic thyroid-stimulating hormone (TSH). • 5. Gonadotrophs: basophilic • follicle-stimulating hormone (FSH) - formation of graafian follicles • luteinizing hormone (LH) I - Induces ovulation & formation of corpora lutea • regulate spermatogenesis & testosterone production in male
Posterior Pituitary • modified glial cells (termed pituicytes) and axonal processes extending from the hypothalamus through the pituitary stalk to the posterior lobe (axon terminals). • oxytocin & antidiuretic hormone (ADH)/ vasopressin
Clinical Manifestations of Pituitary Disease • Hyperpituitarism • Hypopituitarism • Local mass effects - radiographic abnormalities of the sella turcica –EARLIEST - visual field abnormalities - elevated intracranial pressure
Pituitary Apoplexy • acute hemorrhage into an adenoma is associated with clinical evidence of rapid enlargement of the lesion - EMERGENCY
Pituitary Diseases • Primary Tumours • Adenomas • Craniopharyngioma • Metastasis • Empty Sella • Surgical, post-Sheehan’s • Hemorrhage • Sheehan’s syndrome • Hyperfunction • Insufficiency
Pituitary Adenomas • most common cause of hyperpituitarism • classified based on hormone(s) produced - detected by immunohistochemical stains • functional or nonfunctioning • peak incidence 35 to 60 years
Morphology • microadenomas <1 cm macroadenomas >1 cm • soft, well-circumscribed lesion • larger lesions extend through the diaphragm sella into the suprasellar region - compress the optic chiasm & adjacent structures (cranial nerves) • 30% infiltrate neighbouring tissues - invasive adenomas
Acromegaly • growth in skin & soft tissues • viscera (thyroid, heart, liver, adrenals); • bones of the face, hands, feet. • Bone density may be increased (hyperostosis) • Enlargement of the jaw results in protrusion (prognathism), with broadening of the lower face. • broad, sausage-like fingers
Hypopituitarism • Tumors/other mass lesions: exert pressure on adjacent pituitary cells • Trauma & subarachnoid hemorrhage • Pituitary surgery or radiation • Pituitary apoplexy • Sheehan syndrome- postpartum necrosis • Empty sella syndrome - Any condition that destroys almost all of the pituitary gland • Hypothalamic lesions • Inflammatory - sarcoidosis or tuberculous meningitis
Posterior Pituitary Syndromes • Diabetes insipidus. ADH deficiency causes diabetes insipidus, - excessive urination (polyuria) due to an inability of the kidney to resorb water properly from the urine.
Syndrome of inappropriate ADH (SIADH) secretion. ADH excess causes resorption of excessive amounts of free water, resulting in hyponatremia.
ADH by malignant neoplasms (particularly small-cell carcinomas of the lung)
Multiple Endocrine Neoplasia • MEN 1 – Wermersyndrome • Pituitary adenoma (prolactin) • Pancreatic endocrine tumour • Parathyroid hyperplasia(90%)
Multiple Endocrine Neoplasia • MEN 2a – Sipplesyndrome • Medullary thyroid cancer (100%) • Parathyroid hyperplasia (10-40%) • Pheochromocytoma (50%)
Multiple Endocrine Neoplasia • MEN 2b • Medullary thyroid cancer (100%) • Pheochromocytoma (50%) • Ganglioneuromas (100%)