Depression Recognition & Management: Criteria, Incidence & Assessment
280 likes | 297 Views
Understand the criteria, incidence rates, and assessment skills for recognizing and managing depression effectively. Learn the key factors influencing detection, missed diagnosis reasons, and treatment strategies.

Depression Recognition & Management: Criteria, Incidence & Assessment
E N D
Presentation Transcript
Depression Recognition and Management Dr Bruce Davies www.bradfordvts.co.uk
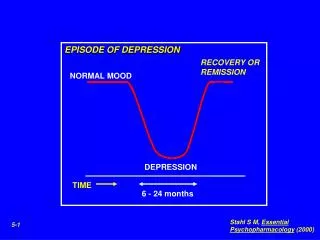
What Is Depression? A Continuum Normal Mood Lowering Abnormal Mood Lowering Abnormal mood lowering and loss of function
What Is Depression? • Depressive disorder • Pervasive • Persistent • Wide range of symptoms
What Is Depression? • Range of symptoms • Negative views • Worthlessness • Incapacity • Guilt • Sleep disturbance • Diurnal mood variation • Loss of energy • Impaired concentration
What Is Depression? • Impaired work ability • Poor social functioning • Psychomotor retardation • Pessimism • Better off dead • Thoughts of suicide • Suicide / action • Fear / belief of bodily illness
Understandability • No longer important. • Do not alter treatment thresholds. • Do not alter treatment. • Reactive / endogenous = confine to bin.
Vulnerabilities • Losses • Stressful life events • Lack of social support • Physical illness • Familial factors • Genetic factors
What Is Depression? - Various Criteria. Defeat Depression Campaign • Depressed mood or loss of pleasure for at least 2 weeks. Plus 4 or more of: • Worthlessness or guilt • Impaired concentration • Loss of energy and fatigue • Thoughts of suicide • Loss or increase of appetite or weight • Insomnia or hypersomnia • Retardation or agitation
What Is Depression? - Various Criteria. DSM – IV • Duration > 2 weeks Depressed mood or Marked loss of interest or pleasure in normal activities • Plus 4 of: • Significant change in weight • Significant change in sleep pattern • Agitation or retardation • Fatigue or loss of energy • Guilt / worthlessness • Can’t concentrate or make decisions • Thoughts of death or suicide
What Is Depression? - Various Criteria. ICD – 10 • Patient has low mood: • How bad is it and how long has it been going on? • Have you lost interest in things? • Are you more tired than usual? If the answer is yes to these, then:
ICD – 10 (Continued) • Have you lost confidence in yourself? • Do you feel guilty about things? • Concentration difficulties? • Sleeping problems? • Change in appetite or weight? • Do you feel that life is not worth living any more?
ICD – 10 (Continued) • Mild. Two criteria from 1-3 and 2 others. • Moderate. Two criteria from 1-3 and 3-4 others or a yes to question 5. • Severe. Most of the criteria in severe form especially questions 5 & 9.
Variants • Depressive episodes that do not meet the criteria for major depression. • Lifelong mild fluctuating depression (Dysthymia). • Mixed states of above two. • Manic depression – bipolar disorder.
Incidence Of Depression : 2000 Patients 100 - major 100 - minor 200 – sub-clinical Depression. In 50% of patients it may not be acknowledged.
Numbers • 10% of those diagnosed in primary care are referred to psychiatrists. • 1 in 1000 are admitted to hospital. • Lifetime incidence rates approach 33%. • 5% of consulters have major depression. • 5% have milder depression. • A further 10% have some depressive features.
Numbers • At least one patient per surgery will have depressive symptoms of some type. • Commoner in younger people including children than thought in the past. • Men:women = 1:2. • Common in the physically ill. • 50% recurrence rate. • 12% become chronically depressed.
Why Missed? • 50% are missed. • 10% subsequently recognised. • Of the 40% who remain unrecognised: • Half remit spontaneously. • Half remain depressed 6 months later.
Missed: Patient Factors • Present somatic symptoms. • Physical problems. • Stigma. • Beliefs about GP role and time to listen. • Longstanding depression. • Less overt / typical. • Less insight.
Missed: Doctor Factors • More accurate doctors. • Make more eye contact. • Show less signs of hurry. • Are good listeners. • Ask questions with social and psychological content. • Less accurate doctors. • Ask many closed questions. • Ask questions derived from theory rather than what the patient just said.
Assessment • Severity • Duration • Social network • Views of self, world and future • Suicidal thoughts • Past history • Factors affecting symptoms • Biological features
Assessment Skills • Directive not closed questions • Picking up on verbal clues “clarification” • Picking up on non-verbal clues and using them • Empathy • Summarising
Treatment Contract • Key skills • Re-frame symptoms as depression • Link to life events • Negotiate anti-depressants if necessary • Problem list and priorities • Set realistic time scale • Agree regular review
Explanations • Depressive illness is clinically different from the blues and involves chemical changes in the brain. • Depressive illness has characteristic symptoms and explain them.
Explanations • Depression benefits from both drug and non-drug approaches. • “Pills for symptoms.” • “Talking for problems.”
Explanations • Anti-depressants are not addictive or habit forming. • Anti-depressants take 2-3 weeks to begin to work and need to be taken for 4-6 months after the full benefit is obtained to prevent relapse.
Explanations • Side effects occur and are expected – explain. • Drugs enable talking therapy to work better. • Regular review is important and needs to continue for at least 6 months.
Explanations • Talking therapy can help solve problems that are soluble, cope with the insoluble and examine other problems that seem unrealistic to the patient or therapist. • Prevention of further trouble will be considered when the treatment is coming to an end.
References • Defeat Depression Campaign. The Royal College of Psychiatrists. 1994. • Treating People with depression: a practical guide for primary care. G Wilkinson et al. Radcliffe 1998. • Recognition and management of depression in general practice: consensus statement. BMJ 1992;305:1198-202.