Download
1 / 22
220 likes | 419 Views
Personality Disorder: A prison perspective. James Taylor Mental Health & Suicide Risk Management Co-ordinator. SPS. Yes, daily. And that’s just the staff!!!. At work do you come into contact with people who have personality disorders?. overview. What are our obligations and aims

E N D
Personality Disorder: A prison perspective James Taylor Mental Health & Suicide Risk Management Co-ordinator. SPS
Yes, daily. And that’s just the staff!!! At work do you come into contact with people who have personality disorders?
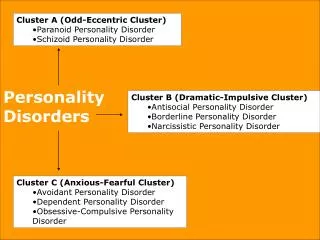
overview • What are our obligations and aims • Prevalence in prisons • A little bit of History • What about today in Scotland’s prisons • Needs v’s diagnosis • Where do we go next?
"The degree of civilization in a society is revealed by entering its prisons.” Dostoyevsky, 19th C
Perspectives • Attitudes • Values • Culture • Environment • Context
SPS –Mission Statement • Custody • Order • Care • Opportunity
Prevalence of personality disorder (from clinical interviews) Singleton et al 1998 Male remand Male sentenced Female Percentage of the population with each type of disorder Type of personality disorder Avoidant 14 7 11 Dependent 4 1 5 Obsessive-Compulsive 7 10 10 Paranoid 29 20 16 Schizotypal 2 2 4 Schizoid 8 6 4 Histrionic 1 2 4 Narcissistic 8 7 6 Borderline 23 14 20 Antisocial634931 Antisocial only 28 30 11 Antisocial and other 35 20 20 Other only 15 15 18 Any personality disorder 78 64 50
Fazel & Danesh 2002 • Large scale systematic review covering • 28 survey examined for PD = 13844 prisoners • 65% male prisoners with PD • 47% ASPD • 42% female prisoners with PD • 21% ASPD
Black et al 2007 • Small study – 220 newly convicted • Nearly 30 % of 220 meet BPD diagnosis • 27% male, • 55% of female (low numbers) • Nearly 57% also ASPD
Darke et al 1998 • 2/3 prisoner on Methadone met diagnosis for ASPD • < 10% diagnosis for Psychopathy • ?Over emphasis on criminal act & related behaviours • The over inclusiveness problem & the under inclusiveness problem
Small/ Special Units • Barlinnie SU, 1973 – 1994 • “A special unit should be provided within the Scottish Penal system for the treatment of known violent inmates, those considered to be violent and selected long term inmates” and • “the traditional officer / inmate relationship should be modified more closely to a therapist / patient basis, while retaining a fair discipline systems”
Historical Management • Between 1992-94 • SPS GiCs noted 100 prisoners unmanageable in mainstream – would suit small unit environment • Jan 1997, 55 prisoner - By 1998, between 60-70. • 1998 Executive Committee for the Management of Difficulty Prisoners formed – continuous assessment for Rule 80 prisoners • 2000 closure of Shotts SU –> management in segregation with individualised regimes
Present Day- ASPD • GPASS 8 records PD unspecified type • From Healthcare 10 in paper records & less than 10 ?Diagnosis • “there are many but nobody likes to document this” • We really don’t know…… • ECMDP – focuses on most challenging
BPD • BPD • “ a pervasive pattern of instability of interpersonal relationships, self image and affects as well as marked impulsivity, beginning by early adulthood and present in a variety of contexts.” DSM-IV-TR
Females in Scottish Prisons • 380 females in custody – 163 (42%) have been managed on ACT2CARE (27% of all males) • 135 recordable incidents of self harm in 2007 (& rising) • Many have evidence of scarring from past lacerations • almost all test positive on admission for substance use • 108 (29%) prescribed methadone. Almost the same again detoxing &
Females in Scottish Prisons 80% history of mental health problems High proportion have history of physical psychological and sexual abuse Significant proportion involved in prostitutions and sex industry Many place little value on their own health needs
Females in custody - BPD In custody- Electronic records = ? 2 Paper records 11 confirmed diagnosis. 2 with ? Diagnosis All +++ self harm 10 substance misuse 10 comorbid other mental illness Another 16 - revolving door – same presentation
Females in custody But why small numbers? Just not recorded in clinical records Only recall most serious examples ? Is it because they are staff intensive 2 requiring 24hr direct 1:1 contact to minimise risk of Self Harm
Need v Diagnosis • “ We just get on with it”, “work with the behaviour” • Management in context • Dynamic risk & needs assessment helps understand behaviour • Behaviour & needs help define the prison ethos, regime & practices
However, diagnosis can matter… • Common terminology • Framework to understand prisoner presentation • Differentiate & define criminogenic and health needs • Obligation to “treat” • Reshaping/enhancing of prison regime • Healthcare (esp. MH) & addictions
Where next for SPS? • Better data collation of current diagnosis • ? Clarification of prevalence • BPD project Cornton Vale • Continue to develop partnerships
So - Why does PD matter? • Impact of the running of the whole prison system. • The need to ensure effective services. • To achieve SPS aims - Rehabilitation, re-integration, care & protection