Download
1 / 26
260 likes | 318 Views
Explore the evolution of epilepsy self-management programs and research collaborations in managing epilepsy well. Learn about innovative online self-management tools, tailored interventions, and the impact of socioeconomic differences on treatment adherence.

E N D
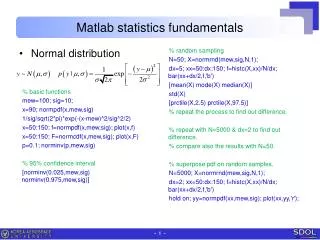
Managing Epilepsy Well (MEW) Research Network (DiIorio et al., 2010) Consumer Generated Self-Management for Adults with Epilepsy (Fraser et al., in press) Review by: Robert Fraser Ph.D., CRC Erica Johnson, Ph.D., CRC
Funding for epilepsy self-management evolved from recommendations from two national conferences, Living With Epilepsy 1 (1993) and Living With Epilepsy 2 (2003), co-sponsored by the Epilepsy Foundation, CDC, etc. • These national meetings highlighted the dearth of evidence-based programs to support self-management in epilepsy vs. widely available programs for those with arthritis, diabetes, or asthma.
LWE-II Priority Recommendationsin Self-Management • Enhancing the Behavioral and Social Science Research relating to epilepsy self-management. • Ensure that programs recognize the spectrum of epilepsy and tailor content (e.g., well-controlled seizures, refractory seizures, etc.). • CDC translated the recommendations into an applied research program.
In 2007, CDC supported the development of the Managing Epilepsy Well Network. First Year of Funding: Emory – the Coordinating Center University of Texas Health Science-Houston Second Year of Funding: University of Michigan University of Washington
Structures of the MEW Network • Four collaborating centers, individual research projects and collaborative projects. • External partners: American Epilepsy Society, Epilepsy Foundation Affiliates, Epilepsy Medical Centers, etc. • Individual research partners: Baker (U.K.), Thorbecke (Germany), etc. with special expertise.
Mission of the MEW Network “To advance the science related to epilepsy self-management by facilitating and implementing research, conducting research in collaboration with network and community partners, and broadly disseminating research findings.”
Emory University’s WebEase • On-line self-management program, based upon social cognitive theory, the trans-theoretical model, and motivational interview. • Three modules (medication, stress, and sleep) and My Log (data tracking system). • Program rated highly as to content and navigability in pilot. Pre-test and post-test demonstrated improvement as to overall self-management, capacity, medication adherence, sleep quality, self-efficacy, and social support.
Emory University’s Project Uplift • Eight module programs delivered weekly through the Internet or by telephone for people with epilepsy wanting to reduce depression. • Combination of cognitive behavioral therapy and mindfulness techniques. • Peer with epilepsy / doctoral student facilitator. • Data now being analyzed – Different modalities vs. wait list control.
University of Texas - Houston Socioeconomic Differences in Epilepsy Self-Management and Its Impact on Treatment Adherence, Health Care Use, and Health Outcomes. • Utilizing a co-hort of 450 patients from 2 socioeconomically diverse Houston clinical sites. • Four quarterly interviews to obtain longitudinal information on their seizure characteristics, knowledge and attitudes about epilepsy, healthcare use, and quality of life. • Additional medical chart review provides information on clinical outcome and medication adherence.
University of Texas - Houston Evaluation of a Clinic-Based Decision Support System. • Mounted on PDA computer accessed by patients and healthcare providers during clinic visits. • Based upon patients’ epilepsy symptoms, behavior, thoughts and beliefs, provides information about patients’ self-management needs, discussion point recommendations, patient management goals, and “action plan” suggestions.
University of Michigan Contributing to Managing Epilepsy Well Phase One: Extensive literature review related not only to epilepsy self-management, but self- management across diverse disabilities. Phase Two: Survey research across 101 key informants who provide or know about evaluated interventions to improve the lives of those with epilepsy.
University of Washington Consumer Generated Self-Management for Adults with Epilepsy • Most self-management models involve a “top down” programmatic approach. • We were desirous of a consumer- generated intervention model.
Managing Epilepsy Well: Needs Assessment Year 1: Evidentiary review to determine seizure, health, psychosocial problems, and well-being variables (prior needs assessments, etc.). Focus group methodology (2 patient groups) to confirm items from evidentiary review, pilot needs assessment survey. Mail survey methodology to collect patient and provider data.
Mail Survey Providers (n = 20; 90+% response rate); Patients (n = 270) from HMC/UWMC, Swedish, EFNW N = 165 surveys returned (61%) Survey methodology important (Dillman et al., 2008): $5 (cash) with physician invitation letter, survey, consent, return SASE $5 (cash) sent upon receipt of survey & consent Hand-addressed & stamped
Mail Survey Seizure information General health information: Perceived well-being; co-morbid conditions Mood and anxiety measures (PHQ, GAD) Life problem rating scales for the following domains: Work Independent living Socializing Epilepsy management Managing emotions and cognition Health and well-being Medical care Self-management program format, leadership, duration, etc. Demographic information
Outpatient Survey Results Average age = 41 years 42% > college degrees 43.6% male 30.7% employed FT, 15.3% PT 23.3% receive disability income due to sz’s Average AED’s = 2.1 (range = 1-9) 79% reported they have a specific sz type 21.5% reported simple partial sz’s 35% reported complex partial sz’s 19% reported secondarily generalized sz’s 44% reported tonic clonic sz’s 8.6% reported myoclonic sz’s 30.7% reported absence sz’s 4.9% reported PNES Seizure Frequency 24.5% haven’t had a sz in 2+ yrs 33.7% have sz’s once/month 18.4% have sz’s 1-3 times/month 11.7% have 1 or more sz’s/week 6.1% have 1 or more sz’s/day
Outpatient Survey Results 36.6% endorse 1+ co-morbid medical conditions. 14.1% endorse 1+ co-morbid neurological conditions. 4.3% endorse 1+ co-morbid sensory conditions. 22.7% endorse 1+ co-morbid emotional/mental health conditions. 40.5% have a lifetime hx of depression tx. 20.9% report current depression tx. 22.7% have lifetime hx of anxiety tx. 12.3% report current anxiety tx.
Outpatient General Survey Results Large within group heterogeneity on problem ratings and the problem ratings are low — why? Are there more homogenous subgroups? Depressed, etc. Preliminary analyses targeted predictors of positive well-being: Perceived health scale Happiness scale Life satisfaction scale
Preliminary Analyses Best correlates of “adjustment” (health, happiness, life satisfaction): Seizure severity Depression Anxiety Income/poverty line Education Cognitive problems
Based Upon Multivariate Linear Progression The best predictor of each adjustment domain was the PHQ-9 depression score alone. As mood decreases, so does health, happiness, and life satisfaction. Second best predictor, indications of cognitive problems, > three of seven.
Secondary Analyses How do people with either… probable major depression, or self-reported cognitive problems …rate their life problems, relative to people without these problems? Probable depression:PHQ-9 > 10. Cognitive problems: Agree/strongly agree that alertness, attention, memory, word finding, multitasking, problem solving, and processing speed are deficient, > three of seven.
Results People with probable major depression or cognitive problems rate virtually all aspects of their life area problems significantly higher than those without. Although there are some problem areas that have salience for both groups.
Self-Management Preferences In-person individual (49%) or group sessions (33%). Meet for 1 hour on a weeknight (55%). Led by a physician or a professional, plus lay person with epilepsy (55%). Educational + emotional coping strategies (42%). Number of sessions, a decided majority < 8 sessions (57%).
MEW Intervention Content • Medical Issues and Epilepsy • Dealing with Sadness and Stress • Assertive Communication and My Disability • Cognition: Memory and Attention • Cognition: Information Processing • Increasing Community Participation • General Health and Well-Being • Managing My Medical Care
Implications Interventionists need to consider direct input from patients/service recipients for tx design. Attention to a more challenged or poorly adjusted subgroup of participants in terms of emotional and cognitive health. Self-management programming may need to be more targeted to optimally serve higher-need groups (while still serving mainstream group). Address life problem areas within the context of mood management and coping?
MEW Network Collaborative Project(s) – Ongoing • Funded by the NIH, Challenge Grant Initiative, Emory is the coordinating center. Utilize Project Uplift materials to “prevent/reduce depression risk” among adults with epilepsy and mild/moderate symptoms. Delivery by telephone or Internet, tested as to efficacy across the four MEW collaborating centers (h = 42 per site). • Self-Management Tool Workgroup