Download
1 / 54
540 likes | 565 Views
Understand the definition, pathophysiology, classification, and treatment of COPD, offering insights into lung function, disease progression, drug classes, and modified treatment approaches as per GOLD guidelines. Learn about the impact of smoking, available therapies, and mortality factors associated with COPD.

E N D
COPD: Risks, Treatment and Mortality Michelle Harkins
COPD: Definition “A disease state characterized by airflow limitation that is not fully reversible….usually both progressive and associated with an abnormal inflammatory response of the lungs…..and systemic manifestations.” ATS Standards for Diagnosis & management of Patients with COPD (2005)
What percentage of smokers develop COPD? A. > 50% B. 30-40% C. 15-20% D. < 10% E. 95%
Lung Function can be improved by smoking cessation. A. True B. False
Which of the following has been shown to improve mortality in COPD? A. Ipratropium B. Salmeterol C. Oxygen D. Lung Volume Reduction Surgery E. Inhaled corticosteroids
COPD Pathophysiology • Airflow obstruction (low FEV1/FVC ratio) is hallmark of COPD • Small airway inflammation & alveolar destruction are the two major pathophysiologic processes • Hyperinflation a major manifestation • ↑ FRC or ↓ IC • Occurs at rest (static) but worsens with exertion (dynamic)
Overall Mechanisms of Cigarette Smoke-Induced Lung Damage Inactivation of antiproteases Oxidative Stress Epithelial permeability Lipidperoxidation Cigarette smoke- derived free radicals and oxidants INJURY Depletion of antioxidantdefenses Antioxidantgenes Neutrophilsequestration Inflammation Transcription of proinflammatory cytokines ‘Susceptibility’ genes MacNee W. Chest. 2000;117:303S-317S.
COPD in the United States Age-Adjusted Death Rates* for COPD by State: 1995-1997 Deaths/100,000 Population Highest 46-61 (11) High 41-45 (13) Low 36-40 (13) Lowest 19-35 (13) *Morbidity and Mortality: 2000 Chart Book on Cardiovascular, Lung, and Blood Diseases. May 2000.
Pulmonary Function in COPD • Spirometry • Decreased FEV1, FEV1/FVC, FEF25-75% • Lung volumes • Increased Total Lung Capacity • Increased Residual Volume • Decreased Vital Capacity due to air trapping • DLCO—decreased in emphysema due to lung destruction
COPD Classification by Severity ** < 50%predicted plus respiratory failure or clinical signs of right heart failure Celli BR, et.al. Eur Respir J 23:932, 2004; Global Initiative for Chronic Obstructive Lung Disease Workshop Report; NHLBI, 2001
Fletcher & Peto Framingham MRC / NOTT Lung Reduction Surgery Anthonosin Laurell and Erickson Lung Health I EROSCOP / LHll Current Guidelines Role of progressive airflow obstruction FEV1 (FVC) is related to all cause mortality Oxygen improves survival Provides minimal improvement Antibiotics for exacerbations Protease / anti-protease Early diagnosis and smoking cessation Steroid use in COPD Long-acting beta-agonists &anticholinergics Major Developments in the Diagnosis and Management of COPD
Accelerated Lung-Function Decline in COPD 100 Nonsmoker 80 COPD 60 Symptoms FEV1 (%) 40 Disability 20 Death 0 20 30 40 50 60 70 80 90 Age (years) Adapted from Fletcher CM, Peto R. Brit Med J. 1977;1:1645-1648.
Average Decrease in FEV1 / year Anthonisen NR, et.al. Am J Respir Crit Care Med 166:675-9, 2002.
Treatment of COPD • Smoking cessation--most important • Oxygen therapy--improves mortality • paO2<55, or 56-59 with pHTN, polycythemia, cor pulmonale • Drugs--help improve symptoms • -agonists, short and long acting • Anticholinergics, short and long acting • Theophylline--may stimulate respiratory center, improve muscle function • Corticosteroids—inhaled, oral • Roflumilast—decreases exacerbations
Classes of Drugs in COPD Albuterol Pirbuterol Levalbuterol SABA Beta-2 agonists Budesonide Fluticasone Mometasone ICS Salmeterol Formoterol Arformoterol Olodaterol LABA SAMA PDEI Ipratropium Roflumilast Theophylline Anti- muscarinics LAMA Tiotropium Aclidinium
Modified Stepwise Approach for COPD Rx (GOLD) Reduce risk factors; Vaccination Pulmonary Rehab O2/ Surgery SABA PRN if respiratory symptoms LAMA LABA ICS, if freq. exac (≥ 2/yr.)
Reduction of Risk Factors: Reduction of personal exposure to environmental risk factors, smoking Fletcher, Peto. Br Med J. 1977, 1:1645
Does Any COPD Drug Improve Health Status? • Yes but barely • Improvement, even when statistically significant, remains clinically modest • Commonest measure of health status used in studies is SGRQ • Change of -4 units is considered clinically relevant
The LEGO Approach for Improving Health Status in COPD Least efficacious Most efficacious ICS LABA ICS LAMA LABA
Does Any COPD Drug Improve Lung Function? • Yes but barely • Improvement, when statistically significant, is clinically modest • MCID is 100 mL • Initial improvement but minimal effect on rate of decline
The LEGO Approach for Improving Lung Function in COPD Least efficacious Most efficacious ICS ICS ICS LABA LAMA LABA LABA LAMA
Does any COPD Drug Confer a Mortality Advantage? • Short answer is NO • But there are nuances • Nothing consistently does so other than oxygen
COPD ManagementOxygen Therapy in Stage IV disease • Improved survival • Prevents progression of PAH • Increases exercise capacity
Summary • Inhaled drugs improve exacerbation rates • Modestly improve health status & lung function • No clear effect on mortality • Combo therapy better than mono therapy for ICS • Triple inhaler therapy is clinically popular but understudied. • Pneumonia risk with ICS • Unclear significance • Roflumilast & chronic macrolides ↓ exac. risk
COPD ManagementPulmonary Rehabilitation Programs • Benefit from exercise training programs • Improved health status • ↑ exercise tolerance & QOL • ↓ dyspnea & fatigue • ↓ hospitalization & LOS • ↓ exacerbations • Improves survival
Acute COPD Exacerbation: Definition • “Acute increase in dyspnea, cough, and/or sputum beyond day-to-day variability, sufficient to warrant a change in Rx” • Important to control • health status; disease progression & mortality ATS Standards for Diagnosis & management of Patients with COPD (2005)
Acute Exacerbations: Classification • Level 1: Treatment at home (optimal) • Level 2: Hospitalization • Sudden increase in symptoms (particularly dyspnea), physical signs, change in mental status • Hypoxemia, hypercapnea • Significant co-morbidities • Elderly • Poor home support • Inadequate response to outpatient therapy • ER visit in last 7-14 days • Level 3: Specialized or ICU care
COPD Management:Acute Exacerbations • Relapse Rate 20-40% • If ER visit : 33% recur within 14 days, 17% eventually need hospitalization • Risk of Relapse • Low FEV1 • Increasing medication use (BDs or steroids) • Prior exacerbations (3 within last 2 years) • Comorbid conditions Miravitlles M, et.al. Factors associated with increased risk of exacerbation and hospital admission in a Cohort of ambulatory COPD patients: a multiple logistics regression analysis. Respiration 67:495, 2000.
Acute COPD Exacerbation: Survival 30-d mortality worse than AMI? Miravitlles M, et.al. Factors associated with increased risk of exacerbation and hospital admission in a Cohort of ambulatory COPD patients: a multiple logistics regression analysis. Respiration 67:495, 2000 Gunen H, Hacievliyagil SS, Kosar F, Mutlu LC, Gulbas G, Pehlivan E, Sahin I, Kizkin O. Eur Resp J. 2005; 26:234-241. .
Acute COPD Exacerbation Treatment • Oxygen: O2 Sat greater than 87% • Bronchodilators: Short Acting B2-Agonists vs Anti-Cholinergics • Similar increase in FEV1 using either alone; data not great for both together except more side effects • Anti-Cholinergics have fewer side effects • MDI (w/ spacer) probably similar to nebulizer if patient can do maneuver • Methylxanthines not very helpful Suto FJ, Varkey B. Current Opinions Pulm Med 9:117-24, 2002
Acute COPD Exacerbations • Corticosteroids • short course improves spirometry, decreases relapse rate • Oral and IV probably equivalent if gut working • 2 week treatment similar to 8 weeks, better than 3 days (IV only) with reduced relapse rate, better gas exchange, spirometry, and DOE • Reduced relapse rate, treatment failure maintained for 6 months (at 6 months no different than placebo; Niewoehner et.al. NEJM 340:1941, 1999) • ? inhaled steroids (few studies in exacerbations, use budesonide)
Low-dose PO Steroids Equally or More Effective as High-dose IV Rx Observational pharmacoepidemiological cohort 414 US hospitals of 79,985 pts. with acute COPD exac. Propensity matching and adjustment to reduce selection bias Low-dose oral steroids: 20-80 mg of oral prednisone daily vs. high-dose IV steroids 120-800 mg prednisone equivalent daily Lindenauer et al. JAMA 201 - 303 (23): 2359 Year
Acute COPD ExacerbationsAntibiotics • Controversial • Greater “success rate” (lower failure rates) when use antibiotics • Anthonisen et.al., Ann Int Med 106:196, 1987 • Adams et.al., Chest 117:1345, 2000 • Daniels et al. AJRCCM 2010 181, 150 • More benefit with worse exacerbation, purulent sputum • “First line” vs. “newer” antibiotics: • ? Fewer treatment failures with 3rd line agents, better cost profile • More studies now taking into account “Exacerbation-Free-Interval” and improved QOL as endpoints (Chodosh S, CHEST 2005; 2231)
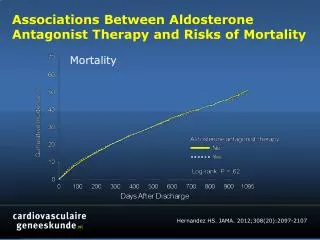
Effect of Abx on Survival Retrospective population-based cohort of 50,000 COPD pts. in Netherlands COPD exac. Rxed with steroids ± abx HR for mortality 0.82 Median time to next exacerbation delayed Roede et al. Thorax 2008: 63:968
COPD Management:NIPPV in Acute Exacerbations • Should be offered if patient remains with respiratory acidosis (pH <7.35) or excessive breathlessness after optimal treatment • If eligible and tolerated (80-85%), shown to be effective and safe for exacerbations with respiratory acidosis (Keenan et.al, 2003): • Decreases symptoms quickly • Decreases hospital stay • Decreases intubation and mortality
COPD Management:NIPPV in Acute Exacerbations • Need to combine CPAP and PSV/EPAP • Improves gas exchange by increasing alveolar ventilation • Improves work of breathing • Exclusion criteria • CV instability • Uncooperative patient • Impaired mental status • Copious secretions / High aspiration risk • Craniofacial abnormalities
NIPPV • Successful in reducing ARF and hospital mortality in DNI patients • Modified and simplified SAPS II and albumin can predict success in DNI pts, above all other variables. • Not successful in patients with hypoxemic AFR or in pt with terminal CA. Schettino et al. Crit Care Med 2005. 33; 1976-1981.
Prolonged Invasive MV • Hospital survival rates for IMV in COPD patients from 31-76% depending on study • One year survival rates from 15-57% • Survival rates 1, 2, 5 yr post IMV at a specialty center: 68%, 54%,and 25% • Inversely assoc. with age, LOS in ICU • NIV may improve survival in selected patients Quinnell et al. Chest 2006; 129: 133- 139.
Difficulty weaning • Muscle weakness (MIP) • Hypercapnia • Malnutrition • Increasing number of exacerbations Nava et al. Eur Respir J 1994 1645-1652
Prognosis and Natural History of COPD • Factors affecting survival • Initial functional impairment • Reversibility of obstruction • Hypoxemia and hypercapnia • Cor pulmonale
FEV1 (L) Prognosis (YRS) 1.4 10 1.0 4 0.5 2 Average Length of Survival Based on FEV1