Download
1 / 46
470 likes | 847 Views
Fad or Function?, Rapid Response Teams (RRT). . by Joel Ray RRT Harborview Medical Center Seattle, WA. Topics of Discussion Understanding the driving forces behind RRT and other patient safety initiatives Getting RRT started at HMC How many calls do we get, and what “triggered” them

E N D
Fad or Function?, Rapid Response Teams (RRT). by Joel Ray RRT Harborview Medical Center Seattle, WA
Topics of Discussion • Understanding the driving forces behind RRT and other patient safety initiatives • Getting RRT started at HMC • How many calls do we get, and what “triggered” them • Improvements for the future
From the “Land Down Under” • Many Australian hospitals instituted “Medical Emergency Teams” (MET) by the mid 1990’s.
Cardiopulmonary Arrest (CPA) • Patients can exhibit clinical warning signs 8-12 hours before event. • Educating acute care staff on identifying clinical triggers and alerting “Code Team”.
What is IHI? • The Institute for Healthcare Improvement(IHI) is a non-for-profit organization leading the improvement of health care throughout the world. IHI was founded in 1991 and is based in Cambridge, Massachusetts
To Error is Human • Despite the extraordinary hard work and best intentions of caregivers, thousands of patients are harmed in US hospitals every day. Hospital-acquired infections, adverse drug events, surgical errors, pressure sores, and other complications are commonplace.
We can do better • Based on data collected over several years from multiple partner institutions, IHI estimates 15 million incidents of medical harm occur in the US each year —a rate of over 40,000 per day. • 400,000 deaths a year world wide.
The Campaign “Planks” --Six Changes That Save Lives • • Deployment of Rapid Response Teams • • Delivery of Reliable, Evidence-Based Care for Acute Myocardial Infarction • • Medication Reconciliation • • Prevention of Central Line Infections • • Prevention of Surgical Site Infections • • Prevention of Ventilator-Associated Pneumonias (VAP)
The 100,000 Lives Campaign Scorecard • An estimated 122,300 lives saved by participating hospitals • Over 3,100 hospitals enrolled • Over 78% of all discharges • Over 78% of all acute-care beds • Over 85% of participating hospitals sending IHI mortality data • Participation in Campaign interventions: • Rapid Response Teams: 60% • AMI Care Reliability: 77% • Medication Reconciliation: 73% • Surgical Site Infection Bundles: 72% • Ventilator Bundles: 67% • Central Venous Line Bundles: 65% • All six: 42%
Possible lives saved – IHI 100,000 Lives Campaign SOURCE: US New & World Report 2005
Washington Hospitals Getting Onboard • Evergreen • Harborview • Overlake • Sacred Heart • Swedish • Tacoma General-Allenmore • Virginia Mason
Topics of Discussion • Understanding the driving forces behind RRT and other patient safety initiatives. • Getting RRT started at HMC. • How many calls do we get, and what “triggered” them. • Improvements for the future
What is UHC? • The University HealthSystem Consortium (UHC), formed in 1984, is an alliance of 97 academic medical centers and 149 of their affiliated hospitals representing nearly 90% of the nation’s non-profit academic medical centers.
HMC’s Initial Process • Conference calls via UHC with other hospitals developing RRT programs. Helped our group anticipate possible stumbling blocks and where to focus energy.
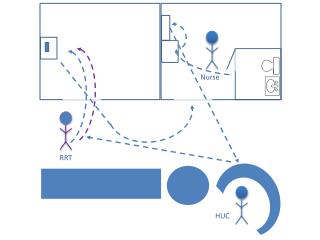
HMC’s Rapid Response Team • Stat RN • Charge Respiratory Therapist • Pulmonary Fellow on MICU (called by RRT with management concerns)
HMC had a head start • Stat RN program started in 1992 as one RN on nights. Currently staffs two RN’s 24/7. Duties include code response, helping ER, units transports. • Dedicated Charge Respiratory Therapist. No individual assignment. Been in place over 2 years. • Can take over 9 months to start RRT program from “scratch”. HMC took 2 months from start to inception.
Some decisions our group made • Cell phones for RRT , help quicken call back time, enhance teams communication with each other. • No overhead pages, It’s not a code, extra sets of eyes not needed. All calls go over pager system. • Clinical Triggers must be resolved before RRT leaves (or ICU transfer) • No “Bogus Calls”, Our goal is to make this process worry free. We want calls to be made.
Advantages of RRT • Much needed resource to acute care RN’s Heavy assignments, new grad’s, are able to see other patients. • Help with triage, facilitate ICU transfer (Pulmonary Fellow ) • Supports acute care RT
“ We are seeing sicker and sicker patients on the floor, they (the RRT) are a great resource.” “They are never threatening. They don’t make you feel stupid. They are great!” Daniel M., RN Burns/Pediatric Unit
“It is a great idea. When a patient doesn’t look right, they can see what is going on and put it into words that will get the doctors to pay attention.” “This has saved lives..” Maryse M., RN Surgery/Trauma Unit
“I just came from the night shift…It prevented a lot of things from going south. It made it a lot easier to call the doctor at 3AM.” Joan M., RN Orthopedics
“ Rapid response has made a real difference. It is much better to get the rapid response page & get people there, rather than hearing about it as a STAT page overhead”.“It frees me up to take care of my other patients”. Lee , RRT HMC
Criteria to remain on Acute floor • Suctioning < q4 hr • FiO2< 50% (exception comfort care) • NPPV; Treatment of OSA (Type 2 intervention).
Multiple RRT’s • Tiers of response First call: Stat RN 1 and Charge RT
Multiple RRT’s • Tiers of response First call: Stat RN 1 and Charge RT Second call: Stat RN 2 and multitasking Charge RT (or next RT to answer my page)
Multiple RRT’s • Tiers of response First call: Stat RN 1 and Charge RT Second call: Stat RN 2 and multitasking Charge RT (or next RT to answer my page) Third call: Nursing Supervisor calls a Charge RN from ICU .
Multiple RRT’s • Tiers of response First call: Stat RN 1 and Charge RT Second call: Stat RN 2 and multitasking Charge RT (or next RT to answer my page) Third call: Nursing Supervisor calls a Charge RN from ICU . Charge Therapist is reviewing retirement information.
Topics of Discussion • Understanding the driving forces behind RRT and other patient safety initiatives. • Getting RRT started at HMC • How many calls do we get, and what “triggered” them. • Improvements for the future
Number of Calls Since Transition Harborview has 369 beds
UCONN UCONN has ~300 beds
HMC RRT Summary • Total calls per month - 93 (average) • Average response time – 4 min (range 1-25 min) • Average call length is 76 minutes • “Third Tier” (ICU RN from unit) activations – 4 times per month • RRT MD Consult – 3 times per month 10-05 to 11-06
The Bottom Line • After the first 1.5 years of Rapid Response, outside the ICU CPA’s are down 7%. (No mortality or bounce back data) • Many other programs are experiencing up to 30% reduction in CPA’s
Topics of Discussion • Understanding the driving forces behind RRT and other patient safety initiatives. • Getting RRT started at HMC • How many calls do we get, and what “triggered” them. • What are the future plans.
RRT Standing orders • Notify Primary Team of Rapid Response Team Activation • Interventions: • - Attach patient to monitor/defibrillator to treat dysrhythmias • - Stat ECG for dysrhythmias / chest pain • - O2 therapy – Titrate FiO2 to maintain SaO2 > 90% • - IV therapy: • Initiate IV therapy if not in place • 1 liter NS bolus for acute blood loss or hypotension • Labs / Tests: • - Chem 7, CBC • - ABG PRN respiratory distress, low SO2, or respiratory concern • - CXR PRN respiratory distress, low SO2, or respiratory concern • - Cardiac enzymes for PRN onset chest pain or dysrhythmias • - Magnesium and ionized calcium PRN new onset dysrhythmias • - Emergency hemorrhage panel PRN evidence of acute hemorrhage • - Type and cross PRN evidence of acute hemorrhage • - Blood culture x2 PRN temp > 39 if no blood cultures in prior 24 hours • - Urine and sputum culture if warranted • Medications: • - Albuterol nebulizers PRN wheezing • - Narcan 0.1 to 0.2 mg IV Q1minute to max of 2 mg PRN altered LOC and documented narcotic administration • (Dilute Narcan in 10 ml NS and administer 1-2 ml every minute until LOC improved)
RRT Standing orders • O2 therapy – Titrate FiO2 to maintain SaO2 > 90% • - ABG PRN respiratory distress, low SaO2, or respiratory concern • - CXR PRN respiratory distress, low SaO2, or respiratory concern • Albuterol nebulizers PRN wheezing
Improved Follow-up • Post Rapid Response Follow Up • - If patient remains on acute care unit after rapid response check vital signs including Temperature, Pulse, BP, RR, Pulse Oximetry and Neuro Check • Q 1h x 2 • Q 2h x 3 • Q 3h x 3 • - Notify Rapid Response Team if the patient meets any of the Clinical Trigger Criteria • PROCESS: • - This document will be given to primary team or RRT MD in the event of an RRT call.
RRT is here to stay • IHI data supports RRT • Activated before emergency occurs. Staff education of clinical triggers essential. • Team consist of ICU RN and RT (MD backup) • Acute care support, “No Bogus Calls”