Download
1 / 35
360 likes | 429 Views
Explore the dangers, pathophysiology, treatment, and complications of caustic ingestion involving acids and alkalis. Learn about grading of injuries, medical pitfalls, specific treatments, and future trends.

E N D
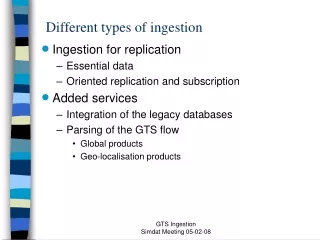
ACID FORMULATIONS • HOUSEHOLD USES Toilet bowel cleaners : sulfuric acid, oxalic acid, carbolic acid Hydro chloric acid, Na bisulphate Drain cleaners : Sulfuric acid Antirust compounds : Phosphoric acid, oxalic acid, Hydrochloric acid, sulfuric acid, chromic Gun bluing agents : Selenious acid Soldering fluxes : Zinc chloride, Hydrochloric acid Automobile battery : Sulfuric acid • INDUSTRIAL USES Above said acids + Hydro fluoric acid
ALKALI FORMULATIONS • Automatic dishwasher – Na metasilicate, detergents Na tripolyPO4, Na Carbonate, • Clinitest tablets -- Cu sulphate, citric acid, Na hydroxide, Na carbonate • Oven cleaners -- Na hydroxide • Bleach products – Na hypochlorite, Na carbonate • Metal cleaners, paint removers, washing powders
OXIDIZING AGENTS • Calcium hypochlorite, hydrogen peroxide, sodium hypochlorite, troclosene sodium and sodium perborate • Oxygen may kill bacteria, and damage living tissue.
PATHOPHYSIOLOGY • Basic cause for injury by either acid or alkali is altering the ionized state, structure of the molecule and disrupting the covalent bonds • Acid causes by hydronium (H +)ions • Alkali does injury by hydroxide (OH) ions
PATHOPHYSIOLOGY ALKALIS SAPONIFICATION OF FAT SOLUBILISATION OF PROTEINS LIQUIFACTION NECROSIS DEEP PENETRATION PERFORATION & STRICTURE ACIDS DENATURE PROTEINS COAGULATION NECROSIS COAGULUM & ESCHAR PREVENTS DEEP PENETRATION
CLINICAL FEATURES • Acids - Stomach Alkali - Pharynx, hypopharynx, esophagus • No correlation between oral injury and internal injury • Dysphagia, drooling, vomiting, haemetemesis, pain and melaena • Hoarseness, stridor and laryngitis indicate impending airway compromise. • Perforation – CV collapse, peritonitis • Significant amount of acid ingestion can cause metabolic acidosis, hemolysis and renal failure.
PHENOL POISONING • Less corrosive • Damages kidney, liver and lung edema • It can cause metabolic acidosis and cardiac depression • Seizures and unconsciousness
GRADINGOF INJURY Grade 1 – Superficial mucosal injury Grade 2 A – Transmucosal injury B – Deep isolated lesions Grade 3 – Full thickness transmural necrosis
APPROACH • HISTORY • EXTERNAL MARKER • X– RAY CHEST & ABDOMEN • ROUTINE INVESTIGATIONS • ABG • ENDOSCOPY 1. 12--24 hrs. may be upto 48 hrs. 2. Determine time to oral feeding and estimation of the risk of stricture& perforation
TREATMENT • Secure airway. If there is stridor or not able to visualize vocal cards, go for tracheostomy. • I.V. access & fluids • Thorough washing of Skin & Eye • Dilution with milk or water can be tried in cases of solid or granular alkali not in acid or liquid alkali. • Dilution is currently not routinely recommended as they induce emesis, obsucer OGD evaluation and increased luminal pressure causing perforation
TREATMENT • ORAL FEEDING 1st degree – 1st day 2A degree – 2-3 day 2B & 3rd degree – Feeding jejunostomy • Antibiotics Reserved for documented infection
CORTICOSTERIODS • Believed to attenuate the inflammation thereby reducing the stricture formation • Some animal studies showed benefits. • However, metanalysis in 1991 and 2004 revealed no benefit of steriods and recommends abandonment of this practice.
MEDICAL PITFALLS • Failure to evaluate and aggressively manage the airway. • Attempting to neutralize the ingested caustic agent with a weak acid or alkaline agent • Inducing emesis • Assuming that the absence of oropharyngeal burns precludes the presence of significant distal injuries
SPECIFIC TREATMENT • Acetic acid – DIC - Cryoprecipitate,FFP • Formic acid - Folinic acid 50 mg. I.V. bolus followed by 1mg/kg 12th hrly • Phosphoric acid - PO4 binders , I.V. glucose, Hydration with normal saline • Hydrofluoric acid - I.V. 10% Ca gluconate 10ml. Then oral Ca tablets 0.5gms.
COMPLICATIONS • Mediastinitis, pericarditis, pleuritis, tracheoesophageal fistula formation, esophageal-aortic fistula formation, and peritonitis. • Delayed perforation - 4 days after an acid exposure • Strictures develop 2-4 weeks postingestion. • Gastric outlet obstruction may develop 3-4 weeks after an acid exposure. • Delayed upper GI bleeding may occur in acid burns 3-4 days after exposure as the eschar sloughs. • Long-term risks include squamous cell carcinoma, which occurs in 1-4 years.
FUTURE TRENDS • Focusing on antioxidant treatment like vitamin E to prevent esophageal strictures. • Ketotofen (mast cell stabilizer) • Phsophatidylcholine which stimulates collagenase activity to prevent excess collagen formation
ETHANOL POISONING • Median lethal dose 5-8g/kg • whiskey-40-60%; wine- 8-16%; rum 40-60% and beer- 3-7% • APPROACH 1. H/o intake & clinical features. 2. Rule out other associated poisonings 3. Look for any injuries like SDH,EDH 4. Ethanol level in all secretions 5. ABG, osmolol gap, anion gap, glucose , electrolytes.
LEVELS & EFFECTS • Intoxication or inebriation - 100-150 mg/dl • Loss of muscle coordination - 150-200 mg/dl • Decreased level of consciousness - 200-300 mg/dl • Death - 300-500 mg/dl
CLINICAL FEATURES • CNS: Depression, disinhibition, ataxia, slurred speech, seizures and unconsciousness • CVS: Myocardial depression, hypotension, arrhythmias, cardiovascular collapse • RS: Depression, aspiration pneumonitis, pul. edema. • ABD: Gastritis, pancreatitis, UGI bleeding • Metabolic : hypoglycemia, lactic acidosis
TREATMENT Secure airway I.V. access 100mg. Thiamine I.V. followed by 50ml. 50% dextrose in comatose pts. Gastric lavage – within 1 hr. Activated charcoal – Coingestants. Alcoholic ketoacidosis – D.N.S. with thiamine and K+ supplements. Hemodialysis
METHANOL • Components Anti-freeze - Gas line & wind shield fluid Fuel - Small hobby machines, Camp stoves Solvents - Paint removers, varnishes Canned fuel , Photocopy fluid. Toxic dose – 40 gms. lethal dose
PHARMACOKINETICS • After ingestion, peak level 30-90 mins. • Hepatic metabolism • Half life is 30 hrs. With ethanol 52 hrs. ADH Methanol Formaldehyde Formic acid H4 Folate CO2 + H2O
CLINICAL FEATURES Effects begin within 1 hr. of ingestion. FORMIC ACID is the main culprit CNS depression, confusion, altered sensorium, ataxia, seizures and unconsiousness. Blurring of vision, diplopia, alteration of colour perception, dilated pupil and absent pupillary response G.I. & Myocardial depression. Sometimes Parkinsonism after long time due to its predilection for basal ganglia.
DIAGNOSIS • Ideal is serum methanol level • H/O intake & clinical features • ABG , anion gap, osmolol gap, electrolytes, renal function tests, CBC.
TREATMENT • GENERAL 1. Induced emesis is not recommended. 2. Secure airway, I.V. access 3. NG suction – 30 mins. 4. pH < 7.3, give NaHCO3
NaHCO3 THERAPY Calculating Requirement (meq) : (15 – HCO3 level) X Wt. (Kg) X 1 50 % of calculated amount as bolus 50 % in 5% D in 4 hours 8.4 % solution – 1 meq Na & HCO3 / ml 7.5 % solution – 0.892 meq Na & HCO3 / ml
ANTIDOTES METHANOL ETHANOL FOMIPEZOLE FORMALDEHYDE Alcohol dehydrogenase FORMIC ACID
INDICATIONS Any one of the following 1. Serum methanol >20mg/dl 2. Documentation of ingestion and residual osmolar gap >10mmol 3. Suspected ingestion with 2 of the following : Arterial pH <7.3 Serum bicarbonate <20mmol/l Osmolar gap >10mmol
DOSE OF ETHANOL • Plasma level should be 100-130 mg/dl. NoviceCh. Alcoholic drinker BOLUS 750 – 1000 mg/kg Maintanance dose 66mg/kg/hr 154mg/kg/hr During dialysis 169mg/kg/hr 257mg/kg/hr It can be given either 10% I.V. or 40% per oral
MONITORING Respiratory depression – ventilatory support Hypoglycemia – Glucose infusion with thiamine Cardiovascular dysfunction Concurrent use of disulfiram like drugs
FOMIPEZOLE 15 mg/kg I.V. – Loading dose 10 mg/kg I.V. 12th hrly 4 doses 15 mg/kg I.V. to counteract metabolism Lesser side effects . Costlier Indications to stop 1. Methanol <20mg/L 2. Normal arterial pH
COFACTOR THERAPY Folinic acid 1mg/kg to max. of 50mg/kg Folic or folinic acid 50mg 4th hrly Alcohol dehydrogenase Methanol Formaldehyde Formic acid H 4 Folate CO2 + H2O
DIALYSIS • High flux Hemodialysis >Peritoneal dialysis • Indications 1. Significant metabolic acidosis pH <7.25 -7.30 2. Abnormalities of vision 3. Deterioration of vital signs despite intensive care 4. Renal failure 5. Electrolyte imbalance 6. Serum methanol >50mg/dl