Download
1 / 32
320 likes | 329 Views
Early psychosis in central Vietnam:. Short-term outcomes and their determinants. First episode psychosis in central Vietnam. Hue University of Medicine & Pharmacy. Student: Seiji Humphries Supervisors: Prof Robert King Prof Michael Dunne Dr Nguyen Huu Cat.

E N D
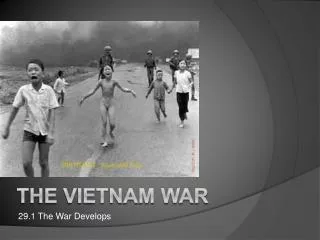
Early psychosis in central Vietnam: Short-term outcomes and their determinants
First episode psychosis in central Vietnam Hue University of Medicine & Pharmacy Student: Seiji Humphries Supervisors: Prof Robert King Prof Michael Dunne Dr Nguyen Huu Cat
Are there better outcomes in LAMIC? WHO International Study of Schizophrenia (>1600 subjects, 12 countries): on average more favourable outcomes in LAMIC – symptoms & functioning, short- & long-term FU Still considerable variation within and between countries Evidence supporting the hypothesis has been hotly contested WHO studies not representative 1 review of 23 LAMIC studies variable outcomes Factors likely to promote poor mental health outcomes: poverty, inequality, stigma, lack of services, staff, education
Gaps in LAMIC Research Still not many longitudinal first-episode psychosis (FEP) studies conducted in diverse LAMIC settings Few LAMIC studies have carefully assessed: 1) Community Functioning; and 2) Subjective Quality of Life (sQOL) Both have become increasingly recognised as an important focus for research and treatment Few LAMIC studies have measured them using sophisticated, multi-dimensional research instruments
Research Questions What are the short-term community functioning and subjective QOL outcomes of people with early psychosis in central Vietnam? What factorsare associated with the outcomes of people with psychotic illness in Vietnam? (Including: clinical symptoms, treatment, demographics, social factors)
Overall Research Timeline Pilot Activities Develop study design, instruments, etc., including interviews with psychiatrists Baseline Assessment of community functioning & sQOL 6-month follow-up Assessment of community functioning & sQOL Mar – Jun 2012, Feb 2013 – Jul 2013 – Jun 2014 Feb – Aug 2014
Main study: Procedure • Chose established research instruments that have been used in cross-cultural studies, especially Asian/LAMIC
Inclusion & Exclusion Criteria Inclusion Criteria 15 – 55 years first episode of a psychotic disorder meeting ICD-10 criteria (F20-F29) within 18 months of study entry; Exclusion criteria: Gross organic cerebral disorder(E.g. ABI, infectious disease) Severe communication difficulties &/or inability to provide informed consent
Sample Referred n= approx.167 Excluded before interview n=68 Interviewed n=99 Excluded after interview n=20 Baseline n=79 Late Entry n=11 Drop out n=11 Follow-up n=57
Community functioning outcomes & associated factors Background: • Single global summary measures may present a distorted picture • Therefore, assess multiple key dimensions of functioning : • occupation • relationships • daily living activities (DLAs) • Functional remission = adequate community functioning • Global functional remission = adequate community functioning in 3 key dimensions
Discussion: remission rates Comparison with other FEP studies challenging
Results: bivariate associations with global community functioning at time 2
Discussion: Factors associated with functional remission Household Economic Status (HES) Household was poor before illness started in many cases Mixed evidence that SES before illness predicts illness course Poverty may affect outcome via poor social support & treatment access, higher unemployment, greater chronic stress Childhood adversity linked to poor outcome Negative symptoms (especially anhedonia) Cognitive symptoms – no relationship with occupational remission because employment is less cognitively demanding?
Discussion: Factors associated with functional remission Poor premorbid functioning – worse odds of adequate global functioning Parent in 2-generation household – better odds of adequate occupational functioning Social support from a ‘special person’ – more support = higher odds of good functioning in daily living activities But maybe more support indicates better social skills?
Subjective QOL & associated factors Background: Subjective QOL very relevant in early psychosis due to high suicide risk Mixed results regarding if QOL improves in 1st few years of illness or not Symptoms (esp. depression) generally predict outcomes Community functioning has weak to moderate relationship with sQOL on average (mixed evidence). Some studies show other factors more important e.g. optimism, self-esteem, self-efficacy Cultural context may influence sQOL
Methods Measure: WHO Quality of Life (abbreviated) scale 4 subscales: physical health psychological social environment
Results & Discussion: sQOL Discussion: Moderate mean sQOL levels but ‘good’ for only a minority Poor QOL for 38% in Environment domain – esp. due to low scores for money & leisure No change for sQOL (or symptoms, support, stigma) but improvement in community functioning Relationships between functioning & sQOL in specific domains are complex e.g. return to work stress, disappointment, compromise
Discussion: Factors associated with subjective QOL Depressed mood & negative symptoms 3/4 domains Positive symptoms & stigma in the Environment domain: socially disruptive behaviour highly stigmatised in Asian countries Community functioning in the Physical Health domain – only large changes are associated with sQOL change Social support (total) all domains: strongest associations were with the Friends subscale, Family subscale showed little variation (mostly high scores) Social support and stigma are both self-rated – may indicate other factors e.g. optimism, self-esteem Marriage 3/4 domains: surprising result may be due to expectations & pressures for older married individuals (vs. young, single individuals)
Limitations Non-Vietnamese researcher Small sample sizes Recruitment process limited sample representativeness Short follow-up period Lack of variation in sample: mode of onset, DUP, medication, family support, type of employment Limited measures of symptom severity and cognitive functioning, none for functional capacity Self-rated measures of social support, stigma experiences Inter-rater reliability was not measured statistically
Significance/Contribution to Knowledge First study of its kind to be conducted in VN; one of very few in LAMIC to rigorously & longitudinally assess functioning/sQOL for early psychosis Multidimensional outcome assessments provide a comprehensive picture Robust estimates of % with adequate community functioning: higher than expected, likely to predict longer term course Importance of factors that determine community functioning may vary according to cultural context: e.g. SES, cognitive symptoms sQOL does not necessarily improve with functioning Factors not related directly to illness, such as economic conditions, can be more important determinants of QOL Cultural context also influences sQOL determinants e.g. marriage
Implications Research Recruitment at Hue hospitals challenging: how to engage more hospital staff in the research? How to recruit participants outside health facilities? More sophisticated measures of symptoms, cognition, functional capacity Treatment Need for targeted interventions: specific dimensions of functioning/sQOL Interventions aimed at functioning cannot be assumed to result in better sQOL Need to account for the sociocultural and economic context Initiatives at community level: peer support; skills training and microfinance loans, use existing community networks; patient, family & worker education
Discussion Questions Why did people from poor households have poorer community functioning? Why did married people have poorer subjective quality of life? Are the results representative of your patients in terms of: duration of untreated psychosis, acute vs extended onset, symptom type and remission, community functioning? Are there any implications for your practice? For the mental health system in Hue?
Xin cảm ơn nhiều! Questions/comments?