Download

1 / 16
160 likes | 277 Views
HIV-infected children born in the UK since 2000 despite maternal diagnosis. National Study of HIV in Pregnancy and Childhood. Claire Townsend UCL Institute of Child Health. NSHPC. HIV-infected children reported in the UK. Children born in the UK to diagnosed women

E N D
HIV-infected children born in the UK since 2000 despite maternal diagnosis National Study of HIV in Pregnancy and Childhood Claire Townsend UCL Institute of Child Health NSHPC
HIV-infected children reported in the UK • Children born in the UK to diagnosedwomen • Children born in the UK to women who were undiagnosed at the time of delivery • Children who were born abroad
Data sources (1) • National Study of HIV in Pregnancy and Childhood (NSHPC) • Surveillance scheme for paediatric and obstetric HIV in the UK and Ireland • Confidential, active reporting schemes • Pregnancies in diagnosed HIV-infected women (RCOG) • Infants born to HIV-infected women (BPSU) • Children followed up to establish infection status • Uninfected: negative PCR after 1 and 3 months of age or negative antibody test.
Data sources (2) • Audit of Perinatal Transmission of HIV in England 2002-2005 • Collaboration between the NSHPC, the Audit Information and Analysis Unit for Specialised Services (AIAU), and CHIVA • Antenatal testing and maternal diagnosis • Pregnancy and HIV management • Social circumstances • Management of delivery • Postnatal details
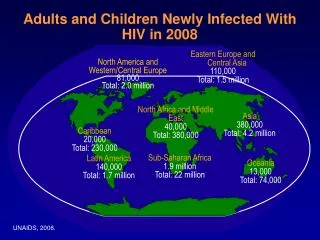
Background – births to HIV infected women (UK and Ireland) • Over 7500 infants born 2000-2007 • Rapid increase in diagnoses of HIV in pregnancy since routine screening promoted • 1200/year since 2005
Uptake of PMTCT interventions (2000-2006) • 97% on ART • 85% HAART • 13% ZDV mono • Of those on HAART • 24% before conception
Trends in uptake of ART and mother-to-child transmission (MTCT) rates, UK and Ireland
61 infected infants born to diagnosed women Total infected infants to date 74 13 - mother received no antenatal ART 8 - mother received <14 days of ART 36 - mother received ≥14 days of ART 3 deliveries <32wks 2 late diagnosis * 3 declined ART 2 deliveries <32wks 5 late diagnosis * 1 late presentation Results • 4 lacked information on ART • 1 late diagnosis • 1 < 32 weeks * Diagnosis <3 weeks before delivery
36 ≥14 days of ART 16 elective CS 8 vaginal 12 emergency CS 6 VL>10,000 (including 1 dual therapy) 10 el CS 3 vaginal remaining 2 mono + VL>50 3 VL>10,000 1 <32 wks 3 32-34 wks 2 VL>10,000 Median duration of treatment: 8 weeks Median gestation at initiation: 30 weeks (IQR: 27-33 weeks) - Concurrent maternal illness / infection - In utero transmission
Perinatal Transmission Audit33 infants born to diagnosed women in England, 2002-2005 • 3 women - labour ward staff were unaware of diagnosis until after delivery • 4 women diagnosed within 2 days of delivery • 3 recent arrivals/visitors, 2 delivered prematurely • 1 confirmed seroconversion in pregnancy • 1 other possible seroconversion
33 infants / diagnosed women • VL>10,000 within 2 weeks of delivery • 36% of women • In utero transmission • 22 infants with early PCR result reported (within 2 days of birth) • 50% had evidence of likely in utero transmission • Social issues • ~ 2/3 of the women had serious problems with immigration status and/or housing • or other major social or mental health problems
33 infants / diagnosed women • Delays • antenatal testing / reporting of results / initiating or changing treatment • Lack of communication between/within Trusts • laboratory / antenatal / HIV care / labour ward • Problems contacting women, women declining care or concealing status • Uncertainty about entitlement to free care
33 infants / diagnosed women • No transmissions were identified following • optimal care and • undetectable maternal viral load at delivery • Only one woman transmitted despite undetectable viral load at delivery • malaria while travelling abroad in early pregnancy • baby PCR positive on day 1 (in utero transmission)
Conclusion • Most transmissions from diagnosed women can be attributed to a combination of factors: • Insufficient maternal ART (often due to prem delivery or late presentation/diagnosis) • Unplanned delivery • High viral load • Audit revealed additional factors: • In utero transmission increasing proportion • Communication issues • Immigration/housing issues
Acknowledgements • Royal College of Obstetricians & Gynaecologists • British Paediatric Surveillance Unit (Royal College of Paediatrics & Child Health) • Respondents to the NSHPC and everyone involved in reporting Funding • Health Protection Agency - NSHPC funding • Medical Research Council - CL Townsend, Training Fellowship Ethics • Multi-centre Research Ethics Committee (MREC/04/2/009) ICH team Principal Investigator: Pat Tookey Additional support: Catherine Peckham, Mario Cortina-Borja Co-ordinator: Janet Masters Researchers: Claire Townsend, Hiwot Haile-Selassie Administrative Assistants: Icina Shakes, Kate Francis Website: www.nshpc.ucl.ac.uk Email: nshpc@ich.ucl.ac.uk NSHPC