Download
1 / 50
650 likes | 3.17k Views
Acid and Base Balance and Imbalance. Mrs. Chaitali Maitra Assistant Professor Dept. of biochemistry PCMS&RC. TO MY STUDENTS HERE I HAVE TRIED TO SIMPLIFY THE HUGE SUBJECT WITH ANIMATIONS, DIAGRAMS, FLOW CHARTS & RELEVENT MCQs. DIFFERENT TEXT BOOKS AND REFERENCE BOOKS HAVE BEEN USED FOR

E N D
Acid and Base Balance and Imbalance Mrs. Chaitali Maitra Assistant Professor Dept. of biochemistry PCMS&RC
TO MY STUDENTS HERE I HAVE TRIED TO SIMPLIFY THE HUGE SUBJECT WITH ANIMATIONS, DIAGRAMS, FLOW CHARTS & RELEVENT MCQs. DIFFERENT TEXT BOOKS AND REFERENCE BOOKS HAVE BEEN USED FOR PREPARING THE CONTENTS. REMEMBERTHESE SLIDES ARE NOT THE SUBSTITUTE OF YOUR TEXT BOOKS ANIMATIONS AND DIAGRAMS ARE COLLECTED FROM DIFFERENT WEBSITE SOLELY FOR EDUCATION PURPOSE.
pH Review • pH = - log [H+] • H+ is really a proton • Range is from 0 - 14 • If [H+] is high, the solution is acidic; pH < 7 • If [H+] is low, the solution is basic or alkaline ; pH > 7
ACID AND BASE • Acids are H+ donors. HCl H+ + Cl- • Bases are H+ acceptors, or give up OH- in solution. KOH K+ + OH- • Acids and bases can be: • Strong – dissociate completely in solution • HCl, NaOH • Weak – dissociate only partially in solution • Lactic acid, carbonic acid H2CO3 H+ + HCO3 -
Ka is an equilibrium constant. For an acid-base equilibrium between a generic acid, HA, and its conjugate base, A−, • HA A− + H+, Ka is defined as • The negative logarithm of the acid dissociation constant (Ka) is the ionisation exponent (pKa) of the acid • pKa = -log Ka • For base, • pKb = -log Kb • Therefore stronger the acid,greater is its ionisation,higher its Ka and lower its pKa.
Or H+ = Ka [HA] [A-] or -log [H+] = -log Ka -log [HA] [A-] Since, pH is negative logarithm of molar concentration of H+ ion to the base 10 and –log Ka=pKa pH = pKa + log [A-] [HA] THE HENDERSON-HASSELBALCH EQUATION When ratio of dissociated and undissociated particle is same i.e. [A-]=[HA] , pH= pKa
BUFFERS ~ buffers are solution which resist any change of pH ~ types mixture of weak acid with their salt and a strong base or mixture of weak base with their salt and a strong acid ~ H2CO3/NaHCO3 (BICARBONATE BUFFER) CH3COOH/CH3COONa (ACETATE BUFFER) ~ buffering capacity of a buffer is defined as the ability of the buffer to resist change in pH when an acid or base is added. ~ How does buffer act?
pH = pKa + log [salt/base] [acid] ~ HENDERSON HESSELBALCH equation gives relationship between pH, pKa, conc. Of acid and conjugate base (or salt), thus when [base/salt]=[acid] ;then pH=pKa. ~ application of the equation 1. determination of pH of buffer solution on addition of salt or acid 2. measurement of concentration of salt and acid by measuring pH. ~ most effective when pH=pKa ,range 1 pH unit higher or lower than pKa.
The Body and pH • Homeostasis of pH is tightly controlled • Extracellular fluid = 7.4 • Blood = 7.35 – 7.45 • < 6.8 or > 8.0 death occurs • Acidosis (acidemia) below 7.35 • Alkalosis (alkalemia) above 7.45
Small changes in pH can produce major disturbances • Most enzymes function only with narrow pH ranges • Tautomeric forms of purine and pyrimidine • Isoelectric pH • pH and excitable tissue • Acid-base balance can also affect electrolytes (Na+, K+, Cl-) • Can also affect hormones
The body produces more acids than bases • Acids take in with foods • Acids produced by metabolism of lipids and proteins sulphuric acid,phosphoric acid ,organic acids • Cellular metabolism produces CO2. • CO2 + H20 ↔ H2CO3↔ H+ + HCO3-
Control of Acids • Buffer systems Take up H+ or release H+ as conditions change Buffer pairs – weak acid and a base Exchange a strong acid or base for a weak one Results in a much smaller pH change
Bicarbonate buffer • Sodium Bicarbonate (NaHCO3) and carbonic acid (H2CO3) • Buffer system of plasma accounts 65% of buffering capacity • Average normal value of HCO3- is24mmol/lit, H2CO3 is1.2mmol/lit,pKa for H2CO3 is 6.1 • Substituting in HH eq. pH = pKa + log[HCO3-/ H2CO3] 7.4=6.1+ log 24/1.2 ratio of 20 • Maintain a 20:1 ratio : HCO3- : H2CO3 • Alkali reserve HCl + NaHCO3↔ H2CO3 + NaCl NaOH + H2CO3 ↔ NaHCO3 + H2O
Phosphate buffer • Major intracellular buffer • Na2HPO4/NaH2PO4 • pKa value is 6.8 • H+ + HPO42-↔ H2PO4- • OH- + H2PO4-↔ H2O + H2PO42-
Protein Buffers • Includes hemoglobin, work in blood and ISF • Carboxyl group gives up H+ • Amino Group accepts H+ • Side chains that can buffer H+ are present on 27 amino acids.
RESPIRATORY REGULATION OF pH • Hemoglobin as buffer • ~N2 of imidazole can give H+ or accepts H+ depending upon pH of the medium. • ~pK of Hb is dependent on oxygenation • ~oxygenated Hb is a stronger acid pKoxy=6.7 • ~Hbdeoxy will take up proton pKdoxy=7.9 • pH influences oxygnation of Hb in lungs and deoxygenation in tissue • acidity of the medium favours delivery of O2 • alkalinity favours oxygenation
Events in lungs and tissue lung tissue HCO3- HCO3- HHb HHb O2 O2 H+ H+ H2CO3 HbO2 HbO2 H2CO3 H2O CO2 H2O CO2 Isohydric transport of co2 EXPIRED AIR METABOLISM
Generation of bicarbonate by RBC LACK OF AEROBIC ACTIVITY,DIFFUSION OF CARBONDIOXIDE,H+ BUFFERED BY HHb.
RENAL MECHANISM FOR REGULATION OF ACID BASE BALANCE ~Buffer system: temporary solution ~Respiratory mechanism provide short time regulation ~Renal mechanism : permanent solution ~Urine pH < plasma pH ,4.5-9.5 ~Eliminate nonvolatile acid, buffered by cation (principally Na+) ~Maintain alkali reserve
CARBONIC ANHYDRASE AND RENAL REGULATION OF pH ~Elimination of nonvolatile acid ~Excretion of H+ ~Occurs in PCT ~Regeneration of bicarbonate ~H+ combine with non carbonate base and excreated
REABSORPTION OF BICARBONATE ~Conservation of bicarbonate ~Urine is free of HCO3- ~Simultaneous excreation of H+
EXCREATION OF TITRABLE ACIDS ~measure of acid excreated by kidney ~no. of millilitres of N/10 NaOH required to titrate 1 litre of urine to pH 7.4 ~role of phosphate buffer
EXCRETION OF AMMONIUM ION NH3 is obtained from deamination of glutamine NH4+ cant diffuse back 2/3 of body acid load liberated in the form of NH4+
Anion gap ~sum of anion and cations is always equal ~sodium and potassium accounts for 95% of cations ~chloride and bicarbonate accounts for 68% of anions ~there is difference between measured anion and cation ~the unmeasured anions constitute the ANION GAP. ~they are protein anions ,sulphates ,phosphates and organic acid ~AG can be calculated as (Na+ + K+)—(HCO3- + Cl-) ~high anion gap acidosis:renal failure,DM ~normal anion gap acidosis:diarrhea ~hyperchloremic acidosis
Acid-Base Imbalances • The body response to acid-base imbalance is called compensation • May be complete if brought back within normal limits • Partial compensation if range is still outside norms. Compensation If underlying problem is metabolic, hyperventilation or hypoventilation can help : respiratory compensation. If problem is respiratory, renal mechanisms can bring about metabolic compensation.
Acidosis • Principal effect of acidosis is depression of the CNS through ↓ in synaptic transmission. • Generalized weakness • Deranged CNS function the greatest threat • Severe acidosis causes • Disorientation • coma Alkalosis • Alkalosis causes over excitability of the central and peripheral nervous systems. • Numbness • Lightheadedness • It can cause : • muscle spasms or tetany • Convulsions • Loss of consciousness
Respiratory Acidosis • Carbonic acid excess caused by blood levels of CO2 above 45 mm Hg. • Hypercapnia – high levels of CO2 in blood • Ratio of bicarbonate/carbonic acid decreased • Chronic conditions: • Depression of respiratory center in brain that controls breathing rate – drugs or head trauma • Paralysis of respiratory or chest muscles • Emphysema • Acute conditons: • Adult Respiratory Distress Syndrome • Pulmonary edema • Pneumothorax
Compensation for Respiratory Acidosis • Kidneys eliminate hydrogen ion and retain bicarbonate ion • Increase NH3 formation • Hyperventilation sets in but removal of co2 is partial as pathogenesis is involved
Respiratory Alkalosis • Carbonic acid deficit • pCO2 less than 35 mm Hg (hypocapnea) • Ratio of bicarbonate/carbonic acid increased • Most common acid-base imbalance • Primary cause is hyperventilation
Respiratory Alkalosis • Conditions that stimulate respiratory center: • Oxygen deficiency at high altitudes • Pulmonary disease and Congestive heart failure – caused by hypoxia • Fever, anemia • Cirrhosis Compensation of Respiratory Alkalosis • Kidneys conserve hydrogen ion • Excrete bicarbonate ion • Decreased excreation of NH3,retention of Cl-
Metabolic Acidosis • Bicarbonate deficit- blood concentrations of bicarb drop below 22mEq/L • Causes: • Loss of bicarbonate through diarrhea or renal dysfunction • Accumulation of acids (lactic acid or ketones) which may occur in DM,starvation,high fever. • Failure of kidneys to excrete H+
Symptoms of Metabolic Acidosis • Headache, lethargy • Nausea, vomiting, diarrhea Compensation for Metabolic Acidosis • Increased ventilation • Renal excretion of hydrogen ions if possible • K+ exchanges with excess H+ in ECF • ( H+ into cells, K+ out of cells)
Metabolic Alkalosis • Bicarbonate excess - concentration in blood is greater than 26 mEq/L • Causes: • Excess vomiting = loss of stomach acid • Endocrine disorders • Heavy ingestion of antacids • Severe dehydration
Compensation for Metabolic Alkalosis • Decreased pulmonary respiration • Increased alkali excreation • Decreased acid excreation • Decreased NH3 formation Symptoms of Metabolic Alkalosis • Respiration slow and shallow • Hyperactive reflexes ; tetany • Often related to depletion of electrolytes • Atrial tachycardia • Dysrhythmias
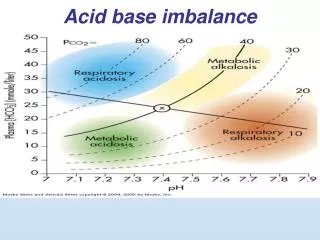
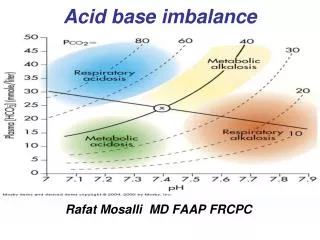
Remember!! When you see “respiratory”, think PCO2 When you see “metabolic”, think [HCO3] • pH = 6.1 +log ([HCO3-]) .03xPCO2
Davenport diagram • Respiratory alkalosis • pH = 6.1 +log ([HCO3-] ) • .03xPCO2
Davenport diagram • Respiratory acidosis • pH = 6.1 +log ([HCO3-] ) • .03xPCO2
Davenport diagram • Metabolic alkalosis • pH = 6.1 +log ([HCO3-] ) • .03xPCO2
Davenport diagram • Metabolic acidosis • pH = 6.1 +log ([HCO3-] ) • .03xPCO2