Download
1 / 120
1.2k likes | 1.24k Views
Explore the use of repetitive transcranial magnetic stimulation (rTMS) in mood, anxiety, psychotic, and substance disorders, focusing on its efficacy in depressive patients and potential applications in other psychiatric conditions.

E N D
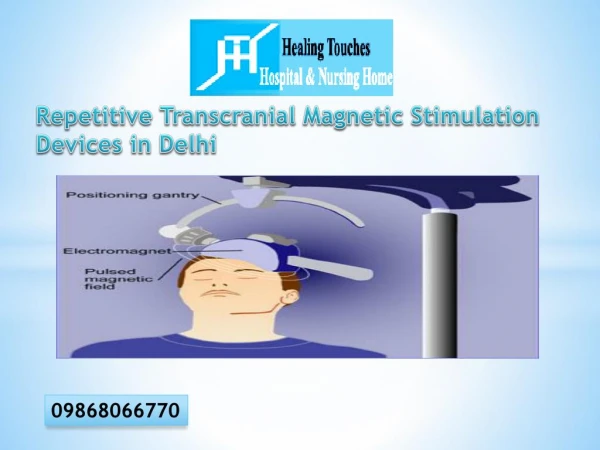
Transcranial Magnetic Stimulation in Psychiatric Disorders Oguz Tan, Memory Center, Istanbul, Turkey
Oguz Tan, Memory Center, Istanbul, Turkey Objectives: It was aimed to review the literature about the clinical use of repetitive transcranial magnetic stimulation (rTMS) therapy in psychiatric disorders. Methods: A medline research was done concerning rTMS use in mood disorders, anxiety disorders, psychotic disorders, and substance use disorders. Results: Application of rTMS in depressive patients usually lead to a significant clinical improvement. Findings about the use of rTMS in manic episodes, anxiety disorders, psychotic disorders, and substance use disorders are limited. Coclusion: rTMS is probably a useful therapeutic tool in depressive disorders. Further research is needed to clarify the role of rTMS in pasychiatric disorders other than depression. Transcranial Magnetic Stimulation in Psychiatric Disorders
Repetitive transcranial magnetic stimulation in the treatment of depression has been intensely studied. Since 1993 until recently, approximately 70 studies evaluating clinical efficacy of rTMS in depression have been published. • Most data support an antidepressant effect of high-frequency rTMS administered to the left prefrontal cortex, although most patients enrolled in the studies had treatment-resistant and severe depression. • Side-effect profile of rTMS is much more favorable than ECT or pharmacotherapy. The only serious side-effect of rTMS is seizure that have occured very rarely.
An important reference is:www.ists.unibe.ch This site contains: The Avery-George-Holtzheimer Database of rTMS Depression Studies UPDATED as of 11/22/2004
SHAM-CONTROLLED STUDIES 33 sham-controlled studies have been conducted since 1993 until June, 2005. 19 out of these studies found that rTMS were superior when compared to sham stimulation. However, in some studies, the benefit from rTMS was modest.
SHAM-CONTROLLED STUDIES 1996 • Pascual-Leone A, Rubio B, Pallardo F, Catala MD • Rapid-rate transcranial magnetic stimulation of left dorsolateral prefrontal cortex in drug-resistant depression. Lancet 348:233-7. • 17 patients. Medication-resistant. Cross-over study. Non medication-free. Psychotic depression.. Left DLPFC 10 Hz Intensity 90 percent MT 5 sessions with active rTMS (cross-over to the other group and five more sessions) Total pulses 10.000 Different cortical areas (vertex stimulation, right DLPFC) stimulation were stimulated. • HAMD decreased from 25.2 to 13.8 after 5 sessions (45 percent decrease in depression)
SHAM-CONTROLLED STUDIES 1997 • George MS, Wassermann EM, Kimbrell TA, et al • Mood improvement following daily left prefrontal repetitive transcranial magnetic stimulation in patients with depression: a placebo-controlled crossover trial. Am J Psychiatry 154:1752-6. • 24 patients. Not medication-resistant. Cross-over study. Some patients are medication-free. Left DLPFC 20 Hz Intensity 80 percent MT 10 sessions Total pulses 8.000 • rTMS superior to Sham, but small decrease in depression rating.
SHAM-CONTROLLED STUDIES 1999 • Avery DH, Claypoole K, Robinson L, et al • Repetitive transcranial magnetic stimulation in the treatment of medication-resistant depression: preliminary data. J Nerv Ment Dis 187:114-7. • 6 patients. Medication-resistant. Not medication-free. Left DLPFC 10 Hz Intensity 80 percent MT 10 sessions Total pulses 10.000 • Slight improvement in rTMS group compared with sham. No decrement in neuropsychological tests with rTMS.
SHAM-CONTROLLED STUDIES1999 • Klein E, Kreinin I, Chistyakov A, et al • Therapeutic efficacy of right prefrontal slow repetitive transcranial magnetic stimulation in major depression: a double-blind controlled study. Arch Gen Psychiatry 56:315-20. 70 patients. Not medication-resistant. Not medication-free. Right DLPFC 1 Hz Intensity 110 percent MT 10 sessions Total pulses 1200 • HAM-D decreased from 25.8 to 13.7 with rTMS and 25.3 to 19.7 with sham. Three dropouts (1 rTMS, 2 sham). Of rTMS patients, 49% were responders (w/ >50% decrease in HAM-D); of sham patients, 25% were responders.
SHAM-CONTROLLED STUDIES 1999 • Loo C, Mitchell P, Sachdev P, McDarmont B, Parker G, Gandevia S • Double-blind controlled investigation of transcranial magnetic stimulation for the treatment of resistant major depression. Am J Psychiatry 156:946-8. • 18 patients. Medication-resistant. Not-medication-free. Left DLPFC 10 Hz Intensity 110 percent MT 10 sessions of real or sham rTMS, then permitted up to 20 sessions of real rTMS Total pulses 15.000 • With rTMS significant decreases in HAMD after 10 sessions, but not different from sham. With rTMS, 44.9% decrease from baseline at one month follow-up.
SHAM-CONTROLLED STUDIES 1999 • Padberg F, Zwanzger P, Thoma H, et al • Repetitive transcranial magnetic stimulation (rTMS) in pharmacotherapy-refractory major depression: comparative study of fast, slow and sham rTMS. Psychiatry Res 88:163-71. • 18 patients. Medication-resistant. Some patients are medication-free. Left DLPFC 10 Hz or 0.3 Hz Intensity 90 percent MT 5 sessions Total pulses 1250 • Not clinically meaningful antidepressant efficacy. Improvement in verbal memory scores after fast rTMS, with no change after slow rTMS, and a trend toward poorer scores after sham.
SHAM-CONTROLLED STUDIES1999 • Kimbrell TA, Little JT, Dunn RT, et al • Frequency dependence of antidepressant response to left prefrontal repetitive transcranial magnetic stimulation (rTMS) as a function of baseline cerebral glucose metabolism. Biol Psychiatry 46:1603-13. • 26 patients. Medication-resistance NA. Some patients medication-free. Left DLPFC 20 Hz or 1 Hz Intensity 90 percent MT 10 sessions Total pulses 8000 • 2/13 responded (greater than 50% response) There was a negative correlation between the degree of antidepressant response after 1 Hz compared to 20 Hz. Better response to 20 hz was associated with the degree of baseline hypometabolism measured by PET, whereas 1 Hz rTMS tended to be associated with baseline hypermetabolism. 1/10 responded in 20 Hz group. 0/3 responded in sham group. Antidepressant response to rTMS might vary as as a function of stimulation frequency and may depend on pretreatment cerebral metabolism.
SHAM-CONTROLLED STUDIES 1999 • Stikhina N, Lyskov EB, Lomarev MP, Aleksanian ZA, Mikhailov VO, Medvedev SV • Transcranial magnetic stimulation in neurotic depression. Zh Nevrol Psikhiatr Im S S Korsakova 99:26-9. • 29 patients. Medication-resistance NA. Medication-free or not NA. All patients received psychotherapy. Left frontal 40 Hz Intensity 0.015 Tesla 10 sessions Total pulses 480.000 • TMS significantly better than control condition.
SHAM-CONTROLLED STUDIES 2000 • Berman RM, Narasimhan M, Sanacora G, et al • A randomized clinical trial of repetitive transcranial magnetic stimulation in the treatment of major depression. Biol Psychiatry 47:332-7. • 20 patients. Medication-resistant. Medication-free. Left DLPFC 20 Hz Intensity 80 percent MT 10 sessions Total pulses 8000 • In rTMS group, 1/10 responded (decrease in HAM-D from 48 to 7); in sham group 0/10 responded. Statistically significant but clinically modest reductions of depressive symptoms.
SHAM-CONTROLLED STUDIES 2000 • Eschweiler GW, Wegerer C, Schlotter W, et al • Left prefrontal activation predicts therapeutic effects of repetitive transcranial magnetic stimulation (rTMS) in major depression. Psychiatry Res 99:161-72. • 12 patients. Not medication-resistant. Medication-free or not NA Left DLPFC 10 Hz Intensity 90 percent MT Crossover study. 4 weeks’ duration consisting of two periods of 5 days with rTMS separated by 9 days of no stimulation Total pulses 20.000 • rTMS significantly better than sham, also used near infrared spectroscopy. Absence of a task-related increase of total hemoglobin concentrations at the stimulation site, but not at other locations, before the first active rTMS significantly predicted the clinical response to active rTMS.
SHAM-CONTROLLED STUDIES 2000 • George MS, Nahas Z, Molloy M, et al • A controlled trial of daily left prefrontal cortex TMS for treating depression. Biol Psychiatry 48:962-70. • 30 patients. Medication-resistant. Medication-free Left DLPFC 5 Hz or 20 Hz or sham Intensity 100 percent MT 10 sessions Total pulses 16.000 • 6/10 responded (greater than 50% decrease in HAMD). 3/10 responded to 20Hz. 0/10 responded to sham.
SHAM-CONTROLLED STUDIES 2001 • Garcia-Toro M, Mayol A, Arnillas H, et al • Modest adjunctive benefit with transcranial magnetic stimulation in medication-resistant depression. J Affect Disord 64:271-5. • 40 patients. Medication-resistant. Not medication-free Left DLPFC 20 Hz 10 sessions Intensity 90 percent MT Total pulses 12.000 • rTMS added to current antidepressant treatments. 5/17 (29%) of patients initially randomized to rTMS were responders (>50% decrease in HDRS). 15 sham non-responders crossed over to receive active 90% MT rTMS; 4/14 (29%) patients that completed 4 weeks of treatment were responders. The 9 non-responders were treated with 10 additional sessions of 110% MT rTMS; 3/9 (33%) were responders. Real, but not sham HF-rTMS, was associated with a significant decrease in the Hamilton Depression Rating Scale, but only twelve patients decreased more than 50%
SHAM-CONTROLLED STUDIES2001 • Szuba MP, O'Reardon JP, Rai AS, et al • Acute mood and thyroid stimulating hormone effects of transcranial magnetic stimulation in major depression. Biol Psychiatry 50:22-7. • 14 patients. Medication-resistance NA. Medication-free NA Left DLPFC 10 Hz Number of sessions NA Intensity 100 percent MT Total pulses NA • No efficacy data presented. Patients receiving active TMS showed greater mood improvements with acute sessions of TMS than patients receiving sham. Subjects are a subset of a larger study evaluation twice daily versus once daily rTMS. The change in TSH from pre- to post-rTMS was significantly different between active and sham sessions
SHAM-CONTROLLED STUDIES 2001 • Manes F, Jorge R, Morcuende M, Yamada T, Paradiso S, Robinson RG • A controlled study of repetitive transcranial magnetic stimulation as a treatment of depression in the elderly. Int Psychogeriatr 13:225-31. • 20 patients. Medication-resistant. Medication-free. Left DLPFC 20 Hz 5 sessions. Intensity 80 percent MT Total pulses 4000 • Studied patients >50 years old (mean age 60.7 years, SD 9.8 years). Neuropsychological testing used MMSE (minimental state examination); no significant difference between groups pre- or post-treatment. 6 responders (3 to rTMS and 3 to sham) had significantly greater frontal lobe volume than non-responders.
SHAM-CONTROLLED STUDIES 2001 • Garcia-Toro M, Pascual-Leone A, Romera M, et al • Prefrontal repetitive transcranial magnetic stimulation as add on treatment in depression. J Neurol Neurosurg Psychiatry 71:546-8. • 28 patients. 16 medication-resistant (a single trial of drug), 12 had not received medication fort he present depressive episode. Patients were started on sertraline. Left DLPFC 20 Hz 10 sessions. Intensity 90 percent MT Total pulses 12.000 • rTMS did not add efficacy over the use of standard antidepressant medication. Studied rTMS versus sham as add-on treatment to sertraline for a major depressive episode. All but two patients received benzodiazepines. Differences in response at 2 weeks in HDRS and BDI, but not at 4 weeks (2 weeks after last treatment). Non-responders to sham were crossed over to receive 90% MT rTMS with identical parameters. Non-responders to active 90% MT rTMS crossed over to receive 110% MT rTMS.
SHAM-CONTROLLED STUDIES 2001 • Lisanby SH, Pascual-Leone A, Sampson SM, Boylan LS, Burt T, Sackeim HA • Augmentation of sertraline antidepressant treatment with transcranial magnetic stimulation. Biol Psychiatry 49:81S. • 36 patients. 61 percent of patients were medication-resistant. Not medication-free. 10 Hz over the left DLPFC or 1 Hz the right DLPFC or sham 10 sessions. Intensity 110 percent MT Total pulses 16.000 • Compared 10 Hz left DLPFC rTMS to 1 Hz right DLPFC rTMS to sham rTMS, all as add-on therapy to sertraline 50 mg. Remission in the active TMS group combined was 25% vs. 8% in the sham group (NS). Degree of medication resistance negatively correlated with response and remission.
SHAM-CONTROLLED STUDIES 2002 • Dolberg OT, Dannon PN, Schreiber S, Grunhaus L • Transcranial magnetic stimulation in patients with bipolar depression: a double blind, controlled study. Bipolar Disord 4:94-5. • 20 patients. Medication-resistance NA. Medication-free NA Left DLPFC Frequency (Hz) NA 10 sessions Intensity NA Total pulses NA • Preliminary report. Response or remission rate NA. Depression decreased 29 percent in the active TMS group, 20 percent in the sham group.
SHAM-CONTROLLED STUDIES 2002 • Padberg F, Zwanzger P, Keck ME, et al • Repetitive transcranial magnetic stimulation (rTMS) in major depression: relation between efficacy and stimulation intensity. Neuropsychopharmacology 27:638-45. • 31 patients. Drug-resistant. Not medication-free. Left DLPFC 10 Hz 10 sessions. Intensity: 100 percent MT or 90 percent MT or sham Total pulses 15.000 MADRS scores: 4% decrease with sham, 15% decrease with 90% MT rTMS, 33% decrease with 100% rTMS. • 3/10 responders (>50% decr in HAMD) and 2/10 partial responders (>25% decr HAMD) with 100% MT rTMS, 2/10 responders and 1/10 partial responder with 90% MT rTMS, 0/10 responders and 2/10 partial responders with sham rTMS. • Patients receiving rTMS had substantially fewer days in the hospital post-treatment (43 days for 100% MT rTMS, 61 days for 90% MT rTMS, 135 days for sham rTMS). Improvement of depressive symptoms after rTMS significantly increased with stimulation intensity across the three groups.
SHAM-CONTROLLED STUDIES 2002 • Boutros NN, Gueorguieva R, Hoffman RE, Oren DA, Feingold A, Berman RM • Lack of a therapeutic effect of a 2-week sub-threshold transcranial magnetic stimulation course for treatment-resistant depression. Psychiatry Res 113:245-54. • 21 patients. Medication-resistant. Not medication-free. Left DLPFC 20 Hz 10 sessions. Intensity: 80 percent MT or sham Total pulses 8000 • No statistically significant difference between rTMS- and sham-treated patients. Authors suggest this may relate to subthreshold rTMS intensity.
SHAM-CONTROLLED STUDIES 2003 • Hoppner J, Schulz M, Irmisch G, Mau R, Schlafke D, Richter J • Antidepressant efficacy of two different rTMS procedures High frequency over left versus low frequency over right prefrontal cortex compared with sham stimulation. Eur Arch Psychiatry Clin Neurosci 253:103-9. • 30 patients. Medication-resistance NA Not medication-free. 20 Hz over the left DLPFC (90 percent MT) or 1 Hz the right DLPFC (110 percent MT) or sham 10 sessions. Total pulses 8000 over the left or 1200 over the right • Patients were started on an antidepressant medication 2 weeks before rTMS, which was used as an add-on treatment. Differences between the rTMS procedures regarding depressive symptoms could not be found.
SHAM-CONTROLLED STUDIES 2003 • Loo CK, Mitchell PB, Croker VM, et al • Double-blind controlled investigation of bilateral prefrontal transcranial magnetic stimulation for the treatment of resistant major depression. Psychol Med 33:33-40. • 19 patients. Drug-resistant. Not medication-free. Bilateral DLPFC 15 Hz 15 sessions. Intensity 90 percent MT Total pulses 27.000 • No significant difference between the two groups. 2 responders in the rTMS groups, 1 responder in the sham group. 6 sham patients crossed over to rTMS; 1 patient in this group responded.
SHAM-CONTROLLED STUDIES 2003 • Nahas Z, Kozel FA, Li X, Anderson B, George MS • Left prefrontal transcranial magnetic stimulation (TMS) treatment of depression in bipolar affective disorder: a pilot study of acute safety and efficacy. Bipolar Disord 5:40-7. • 23 patients. Drug-resistance NA Not medication-free. Left DLPFC 5 Hz 10 sessions. Intensity 110 percent MT Total pulses 16.000 • No significant difference between rTMS and sham in decrease in HAMD or response rate. No patients developed mania or hypomania during the study.
SHAM-CONTROLLED STUDIES2003 • Herwig U, Lampe Y, Juengling FD, et al • Add-on rTMS for treatment of depression: a pilot study using stereotaxic coil-navigation according to PET data. J Psychiatr Res 37:267-75. • 25 patients. Some patients are drug-resistant. Not medication-free. 6 parients were given left DLPFC, 6 right, 6 sham (parietooccipital) 15 Hz 10 sessions. Intensity 110 percent MT Total pulses 30.000 • Real stimulation improved depression moderately but significantly better compared to sham. In the real condition, four out of 13 patients responded, whereas none responded to sham. Left vs. right prefrontal location of stimulation guided by PET-identified prefrontal hypometabolism (when present). 11 of 25 patients had right prefrontal hypometabolism at baseline. 1 of 25 had left prefrontal hypometabolism at baseline. 13 of 25 had left=right metabolism at baseline or no imaging data available. There was no evidence that using baseline prefrontal hypometabolism to guide treatment location was beneficial. Treatment groups were combined for analyses.
SHAM-CONTROLLED STUDIES2003 • Nahas Z, Kozel FA, Li X, Anderson B, George MS • Left prefrontal transcranial magnetic stimulation (TMS) treatment of depression in bipolar affective disorder: a pilot study of acute safety and efficacy. Bipolar Disord 5:40-7. • 23 patients. Medication-resistance NA. Not medication-free. Left DLPFC 5 Hz 10 sessions. Intensity 110 percent MT Total pulses 16.000 • No significant difference between rTMS and sham in decrease in HAMD or response rate. But a trend for greater improvement in daily subjective mood ratings. No patients developed mania or hypomania during the study.
SHAM-CONTROLLED STUDIES 2003 • Fitzgerald PB, Brown TL, Marston NA, Daskalakis ZJ, De Castella A, Kulkarni J • Transcranial magnetic stimulation in the treatment of depression: a double-blind, placebo-controlled trial. Arch Gen Psychiatry 60:1002-8. • 60 patients. Medication-resistance NA. Not medication-free. 3 groups: 1-10 Hz left DLPFC 2-1 Hz right DLPFC 3-Sham 10 sessions. Intensity 100 percent MT Total pulses 3000 or 10.000 • Compares 10 Hz LPF stim with 1 Hz RPF stim with sham. Initial trial was with 10 sessions: 14-15% decr in MADRS in both rTMS groups (1/20 patients in LPF group with >50% decr), 1% decr in sham (significant difference between the treatment and sham groups, but not significant difference between the treatment groups). 15 patients with >20% decr in MADRS by 10 sessions went on to receive a total of 20 open rTMS sessions: 40% decr in MADRS in LPF group (4/8 patients with decr >50%), 57% decr in RPF group (4/7 patients with decr >50%). Baseline psychomotor agitation predicted succesful response to treatment.
SHAM-CONTROLLED STUDIES2004 • Hausmann A, Kemmler G, Walpoth M, et al • No benefit derived from repetitive transcranial magnetic stimulation in depression: a prospective, single centre, randomised, double blind, sham controlled "add on" trial. J Neurol Neurosurg Psychiatry 75:320-2. • 41 patients. Medication resistance NA. They were medication-free, medication started at the start of rTMS. Group 1: 20 Hz over the left DLPFC and subsequent sham 1 Hz over the right DLPFC Group 2: simulataneous bilateral active stimulation (20 Hz over the left DLPFC, 1 Hz over the right DLPFC) Group 3: bilateral sham stimulation Intensity 100 percent motor threshold in the 20 Hz group, 120 in the 1 Hz group 10 sessions Total pulses 20.000-26.000 • No significant differences between the groups. 20 Hz LPF and the combined 20 Hz LPF/1 Hz RPF active rTMS groups were combined for efficacy analyses. Unknown if patients were treatment-resistant at baseline. The results suggest that rTMS as an "add on" strategy, applied in a unilateral and a bilateral stimulation paradigm, does not exert an additional antidepressant effect.
SHAM-CONTROLLED STUDIES2004 • Jorge RE, Robinson RG, Tateno A, et al • Repetitive transcranial magnetic stimulation as treatment of poststroke depression: a preliminary study. Biol Psychiatry 55:398-405. • 20 patients. Drug-resistant. Medication-free. Left DLPFC 10 Hz 10 sessions. Intensity 110 percent MT Total pulses 10.000 • 3 patients in the active rTMS group responded and one patient remitted, no patients in the sham group responded. 38 percent decrease in depression in the active rTMS group, 13 percent in the sham group.
SHAM-CONTROLLED STUDIES 2004 • Holtzheimer PE, 3rd, Russo J, Claypoole KH, Roy-Byrne P, Avery DH • Shorter duration of depressive episode may predict response to repetitive transcranial magnetic stimulation. Depress Anxiety 19:24-30. • 15 patients. Drug-resistant. Medication-free. Left DLPFC 10 Hz 10 sessions. Intensity 110 percent MT Total pulses 16.000 • No significant difference between rTMS and sham; however, a significant negative correlation between length of current depressive episode and response to rTMS was found. Non-responders to sham were allowed to receive active rTMS. Patients with a current episode shorter than 4 years showed a 52% reduction in mean HAM-D whereas those with a current episode longer than 10 years showed only a 6% decrease.
SHAM-CONTROLLED STUDIES 2004 • Kauffmann CD, Cheema MA, Miller BE • Slow right prefrontal transcranial magnetic stimulation as a treatment for medication-resistant depression: a double-blind, placebo-controlled study. Depress Anxiety 19:59-62. • 12 patients. Drug-resistant. Not medication-free. Right DLPFC 10 Hz 10 sessions. Intensity 110 percent MT Total pulses 1200 • No significant difference between the groups. However, the active TMS group showed a significant reduction in HAMD over time whereas the sham group did not. Active TMS responders relapsed in 2-3 months. Sham responders relapsed in 2 weeks.
SHAM-CONTROLLED STUDIES2004 • Mosimann UP, Schmitt W, Greenberg BD, et al • Repetitive transcranial magnetic stimulation: a putative add-on treatment for major depression in elderly patients. Psychiatry Res 126:123-33. • 24 elderly patients (mean age 62 years). Drug-resistant. Not medication-free. Left DLPFC 20 Hz 10 sessions. Intensity 100 percent MT Total pulses 16.000 • No additional antidepressant effect of active rTMS.
SHAM-CONTROLLED STUDIES2004 • Fregni F, Santos CM, Myczkowski ML, Rigolino R, Gallucci-Neto J, Barbosa ER, Valente KD, Pascual-Leone A, Marcolin MA. • Repetitive transcranial magnetic stimulation is as effective as fluoxetine in the treatment of depression in patients with Parkinson's disease. J Neurol Neurosurg Psychiatry. 2004 Aug;75(8):1171-4. • 42 patients. Not medication-resistant. Not medication-free. 15 Hz 10 sessions. Group 1: active rTMS and placebo drug treatment Group 2: sham rTMS and fluoxetine 20 mg/day. • Depression scores were improved to the same extent in both groups after two weeks of treatment (HDRS 38% for group 1, 41% for group 2). At week 8 there was a tendency for worse motor UPDRS (Unified Parkinson’s Disease Rating Scale) scores in group 2. ADL (Acitivities of Daily Living) showed improvement at week 8 only in group 1. MMSE (Minimental State Examination) improved in both groups after treatment, but faster in group 1 than in group 2. There were fewer adverse effects in group 1 than in group 2. rTMS has the same antidepressant efficacy as fluoxetine and may have the additional advantage of some motor improvement and earlier cognitive improvement, with fewer adverse effects.
SHAM-CONTROLLED STUDIES2004 • Koerselman F, Laman D, van Duijn H, van Duijn M, Willems M • A 3-month, follow-up, randomized, placebo-controlled study of repetitive transcranial magnetic stimulation in depression. J Clin Psychiatry 65(10):1323-1328. • 55 patients. Drug-resistance NA. Not medication-free. Left DLPFC 20 Hz 10 sessions. Intensity 80 percent MT Total pulses 8000 • No difference between active and 45 deg sham TMS after 2 weeks of treatment. However, at 12 weeks, the active TMS group was significantly less depressed than the sham group.
SHAM-CONTROLLED STUDIES2005 • Rumi DO, Gattaz WF, Rigonatti SP, Rosa MA, Fregni F, Rosa MO, Mansur C, Myczkowski • ML, Moreno RA, Marcolin MA. Biol Psychiatry. 2005 Jan 15;57(2):162-6. • Transcranial magnetic stimulation accelerates the antidepressant effect of amitriptyline in severe depression: a double-blind placebo-controlled study. • 46 patients All patients were concomitantly taking amitriptyline (mean dose 110 mg/day). Left DLPFC 5 Hz 20 sessions Intensity 120 percent MT Total pulses 25.000 • rTMS had a significantly faster response to amitriptyline. There was a significant decrease in HAM-D/17 scores, already after the first week of treatment compared with sham. The decrease in HAM-D/17 scores in the rTMS group was significantly superior compared with the sham group throughout the study (p < .001 at fourth week).
rTMS versus ECT Since 2000 until today, 7 studies comparing rTMS with ECT and some case reports have been publishes. In non-psychotic depression, it was found that the efficacy of rTMS was nearly equal to that of ECT, with a much more favorable side-effect profile.
rTMS versus ECT 2000 • Grunhaus L, Dannon PN, Schreiber S, et al • Repetitive transcranial magnetic stimulation is as effective as electroconvulsive therapy in the treatment of nondelusional major depressive disorder: an open study. Biol Psychiatry 47:314-24. • 40 patients referred for ECT rTMS group medication-free. Left DLPFC 10 Hz Intensity 90 percent MT 20 sessions Total pulses 8000 • 7/16 responded to rTMS;12/18 to ECT. Among nonpsychotic depressed 5/8 responded to rTMS; 5/10 to ECT. Among psychotically depressed, only 2/8 responded to rTMS; 7/8 to ECT.
rTMS versus ECT 2000 • Pridmore S. • Substitution of rapid transcranial magnetic stimulation treatments for electroconvulsive therapy treatments in a course of electroconvulsive therapy. Depress Anxiety. 2000;12(3):118-23. • 22 patients Randomized, single-blind, controlled study. Two streams were conducted: Stream 1 received non-dominant unilateral (UL) ECT only, treatments being given 3 times per week for 2 weeks (11 patients). Stream 2 received a combination of treatments: one UL ECT on Day 1 and rTMS on the following 4 days, all repeated once, after a 2-day respite (11 patients). • There was no evidence that the antidepressant effect of the ECT only stream was superior to that of the ECT plus rTMS stream. There was no increase in subjective side-effects in the ECT plus rTMS stream. On the contrary, this stream was accompanied by less side effects than the ECT only stream in this study.
rTMS versus ECT 2000 • Pridmore S, Bruno R, Turnier-Shea Y, Reid P, Rybak M • Comparison of unlimited numbers of rapid transcranial magnetic stimulation (rTMS) and ECT treatment sessions in major depressive episode. Int J Neuropsychopharmacol 3:129-134. • 32 patients. Medication-resistant. Not medication-free. Left DLPFC 20 Hz Intensity 100 percent motor threshold 10-16 sessions (until remission occurred or response plateaued) Total pulses 10.000-16.000 • Gave unlimited number of rTMS sessions (mean 12.2, SD 3.4). Compared to group of 16 patients receiving unlimited ECT treatments (mean 6.2, SD 1.6). No significant difference between the groups in HDRS improvement. Patients receiving ECT had significantly greater decrease in Beck Depression Inventory scores. A significant main effect for treatment type was found [Pillai trace = 0.248, F(3,28) = 3.076, p = 0.044; power = 0.656], reflecting an advantage for ECT patients on measures of depression overall, however, rTMS produced comparable results on a number of measures. Blind raters using the 17-item Hamilton Depression Rating Scale (HDRS) found the rate of remission (HDRS = ? 8) was the same (68.8%), and the percentage improvement over the course of treatment of 55.6% (rTMS) and 66.4% (ECT), while favouring ECT, was not significantly different. Significant differences were shown (p & 0.03) in percentage improvement on Beck Depression Inventory ratings (rTMS, 45.5%; ECT, 69.1%), but not for improvement in Visual Analogue ratings of mood (rTMS 42.3%; ECT, 57%).
rTMS versus ECT2001 • Smesny S, Volz HP, Liepert J, Tauber R, Hochstetter A, Sauer H. • Repetitive transcranial magnetic stimulation (rTMS) in the acute and long-term therapy of refractory depression--a case report]. Nervenarzt 2001 Sep;72(9):734-8 • A patient with therapy-resistant major depression has been hospitalized for 60 months during the last 7 years. • Not even five electroconvulsive therapy (ECT) series (61 single applications) brought lasting remission of symptoms. As cognitive deficits developed and prolonged postnarcotic recovery times were observed, further ECT was contraindicated. • (rTMS) to the left frontal cortex • Only a few rTMS applications already caused an obvious brightening in mood, remission of depressive delusional symptoms, and an increase in personal interests and activities. After 4 weeks of daily treatment, the patient was discharged from the ward. The rTMS treatments and psychotherapeutic counseling have been continued on an outpatient basis. Thus, pharmaco- and psychotherapeutic interventions combined with rTMS led to persistent symptom remission and social reintegration.
rTMS versus ECT 2001 • Dannon PN, Grunhaus L. • Effect of electroconvulsive therapy in repetitive transcranial magnetic stimulation non-responder MDD patients: a preliminary study. Int J Neuropsychopharmacol. 2001 Sep;4(3):265-8. • The aim was to measure the effectiveness of ECT in-patients who had failed to respond to a course of repetitive transcranial magnetic stimulation (rTMS) treatment. • 17 patients with severe MDD who had not responded to a course of rTMS were switched to receive ECT treatments. • 7 out of 17 patients responded to ECT. (3 out of 5 non-psychotics and 4 out of 12 psychotic patients). • ECT seems to be an effective treatment for 40% of patients who failed to respond to rTMS treatment. • Whether this is a result of reduced responsiveness to ECT in rTMS-resistant patients or a consequence of small sample size requires further study.
rTMS versus ECT2001 • Hasey G. • Transcranial magnetic stimulation in the treatment of mood disorder: a review and comparison with electroconvulsive therapy. Can J Psychiatry. 2001 Oct;46(8):720-7. • The potential for unwanted side effects is substantially reduced, compared with ECT. • In open trials, rTMS and ECT are reported to be equally efficacious for patients having depression without psychosis. • But the therapeutic benefits reported in double-blind sham-rTMS controlled trials are more modest.
rTMS versus ECT2002 • Janicak PG, Dowd SM, Martis B, et al • Repetitive transcranial magnetic stimulation versus electroconvulsive therapy for major depression: preliminary results of a randomized trial. Biol Psychiatry 51:659-67. • 25 patients. Medication-resistant. Not medication-free. Left DLPFC 10 Hz Intensity 110 percent motor threshold 10-20 sessions Total pulses 10.000-20.000 • Patients received either rTMS or bitemporal ECT (4-12 treatments). There was a raw difference in mean change in HDRS between the groups (55% with rTMS, 64% with ECT), but no statistically significant difference. There was a 46% response rate with rTMS and a 56% response rate with ECT (not statistically significant).
rTMS versus ECT 2002 • Dannon PN, Dolberg OT, Schreiber S, Grunhaus L. • Three and six-month outcome following courses of either ECT or rTMS in a population of severely depressed individuals--preliminary report. Biol Psychiatry. 2002 Apr 15;51(8):687-90. • 3- and 6-month outcomes of a group of patients treated with either ECT (n = 20) or (rTMS) (n = 21). • With or without psychotic features referred for ECT • Forty-one patients who responded to either treatment constituted the sample. • Medications were routinely prescribed. • There were no differences in the 6-month relapse rate between the groups. • Overall, 20% of the patients relapsed (four from the ECT group and four from the rTMS group). • Patients reported equally low and not significantly different scores in the HRSD (ECT group 8.4 +/- 5.6 and TMS group 7.9 +/- 7.1) at the 6-month follow up. • The clinical gains obtained with rTMS last at least as long as those obtained with ECT.
rTMS versus ECT 2003 • Grunhaus L, Schreiber S, Dolberg OT, Polak D, Dannon PN • A randomized controlled comparison of electroconvulsive therapy and repetitive transcranial magnetic stimulation in severe and resistant nonpsychotic major depression. Biol Psychiatry 53:324-31. • 41 patients with nonpsychotic MDD referred for ECT Not medication-free. Left DLPFC 10 Hz Intensity 90 percent motor threshold 20 sessions Total pulses 24.000 • No significant difference in HDRS decrease between rTMS and ECT patients. 12/20 ECT responders and 11/20 rTMS responders (>50% decr in HDRS, final HDRS <10); no significant difference between groups). 30% remission rate (final HAMD<9) in ECT and rTMS groups. For ECT group, patients received unilateral ECT initially, then bilateral ECT if no response after 6 treatments; 13 patients received unilateral ECT, 7 received bilateral ECT -- no significant difference in response rate between these groups.
rTMS versus ECT2004 • Conca A, Hrubos W, Di Pauli J, Konig P, Hausmann A. • ECT response after relapse during continuation repetitive transcranial magnetic stimulation. A case report. Eur Psychiatry. Apr;19(2):118-9. • A woman who exerted a recurrent moderate major depressive episode, 6 months after discontinuation of maintenance ECT. She responded to acute rTMS treatment which was followed by the rTMS maintenance-protocol. Within 2 months of continuation rTMS she relapsed suffering from a severe non psychotic depressive episode and had to be switched to a successful ECT. In this patient rTMS had a good clinical impact as an acute treatment strategy, but failed to prevent relapse as the continuation ECT previously did in the same patient.
rTMS versus ECT 2004 • Kozel FA, George MS, Simpson KN. • Decision analysis of the cost-effectiveness of repetitive transcranial magnetic stimulation versus electroconvulsive therapy for treatment of nonpsychotic severe depression. CNS Spectr. Jun;9(6):476-82.Compared the costs of three different treatment strategies for nonpsychotic severe depression. 1-ECT alone • 2-rTMS alone • 3-rTMS followed by ECT for nonresponders (rTMS-to-ECT). • Calculated 12-month costs and quality adjusted life years (QALYs) for the three treatment options for all nonpsychotic, severely depressed United States patients who would have otherwise undergone ECT. • The additional cost of using ECT alone compared with rTMS alone was 460,031 US dollars per quality adjusted year of life gained. For ECT versus rTMS-to-ECT, there was both an increased cost and a loss of 1,538 QALYs with ECT alone. • If rTMS were to be made widely available clinically in the US, it would offer a substantial economic benefit over ECT in treating resistant depression. Using rTMS-to-ECT offers not only an economic advantage but also an increase in QALYs.