Download
1 / 32
330 likes | 631 Views
Epidemiology of preterm birth. Stefan Johansson Department of Neonatology, Karolinska university hospital Department of Medical Epidemiology and Biostatistics, Karolinska institutet Stockholm, Sweden. extremely preterm ≤ 27 weeks. term 37-41 weeks. postterm ≥ 42 weeks. very preterm

E N D
Epidemiology of preterm birth Stefan Johansson Department of Neonatology, Karolinska university hospital Department of Medical Epidemiology and Biostatistics, Karolinska institutet Stockholm, Sweden
extremely preterm ≤ 27 weeks term 37-41 weeks postterm ≥ 42 weeks very preterm 28-31 weeks moderately preterm 32-36 weeks Preterm birth preterm ≤ 36 weeks Stefan Johansson
Preterm birth - not uncommon • extremely preterm 500 per year • very preterm 1500 • moderately preterm 4500 Stefan Johansson
Preterm birth - part of being human? • Preterm birth more common in humanscompared to other mammalian species. • Evolutionary trend towards earlier birth? • narrow pelvis related to bipedal gait • large brain / head and risk of obstructed labour Steer. BJOG 2005;112, S1:1 Stefan Johansson
Preterm birth ≠ prematurity • Preterm birth refers to the timing of birth. • Prematurity refers to immature organ systems at birth. • Most infants born in week 35-36 are ”mature” and cared for in regular maternity units. • infants born at term (37 weeks and onwards) can suffer from some degree of immaturity Stefan Johansson
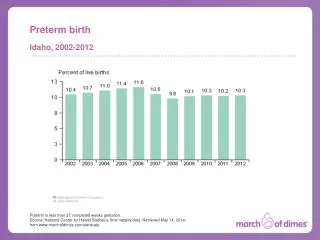
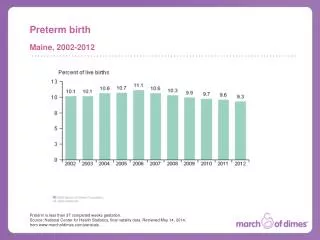
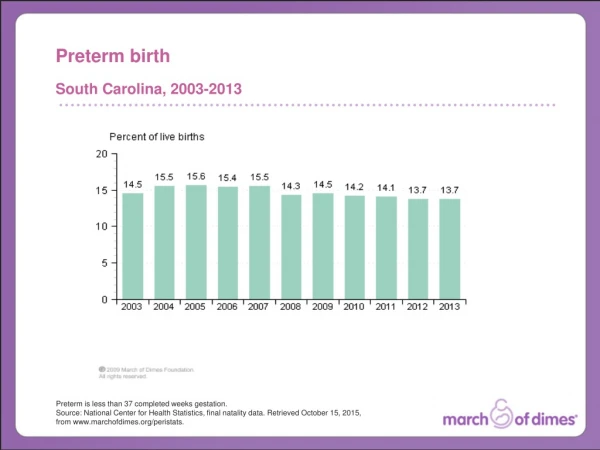
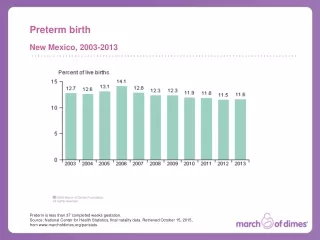
Rates of preterm birth varies in the world • Sweden 6 % • US 10 % • Malawi 22 % • Why do ratesvary? Stefan Johansson
Increasing rates of preterm birth • Due to factors such as • in vitro fertilization • higher maternal age • Induced delivery before term • ultrasound dating of pregnancy length • However, among Danish ”low risk” women the rate of preterm delivery has increased by 51% from 1995 to 2004,from 3.8 to 5.7% • why?? Langhoff-Roos. BMJ 2006;332:937 Stefan Johansson
Preterm birth and mortality - world-wide • One million infants born preterm die during the first four weeks (26% of neonatal mortality). Lawn et al, Lancet 2005;365:891-900 Stefan Johansson
Gestational age and mortality - Sweden Perinatal mortality (%) in Sweden 2003, by gestational age. Stefan Johansson
Very preterm birth and mortality - Sweden Infant mortality (%) in Sweden 1992-98, by gestational week Stefan Johansson
Methodological problems - gestational length • How is gestational length defined? • last menstrual period • early ultrasound (measuring bones, head and abdomen) Stefan Johansson
Methodological problems - gestational length • Gestational length, based on last menstrual period (LMP) • true gestational length is shorter • the rate of preterm birth is underestimated • Gestational length, based on ultrasound • more exact • unavailable in most countries Stefan Johansson
Methodological problems - preterm birth • What is the method of assessing gestational length? • Which preterm born infants are classified as alive / dead? • ”live-born infants”? • ”still-births”? • Border of viability and neonatal care policies? • Live-born infants>23-24 wks can be admitted to neonatal care. • The policy regarding which infants to treat vary between countries. Stefan Johansson
Methodological problems - preterm birth • Rates of preterm birth and maternal and obstetric care • is expected day of delivery (i.e. 40 completed weeks) calculated? • are birth date recorded and gestational length calculated? • are those data registrered? Stefan Johansson
Methodological aspects of mortality • Consistent definition of outcome… • Consensus on definitions: • Perinatal mortality stillbirths + death during the first week • Neonatal mortality during the first four weeks • Infant mortality during the first year Stefan Johansson
Methodological aspects of mortality • How is ”alive” determined at birth? • How are deaths recorded? • Mortality rates of live-born preterm infans underestimate the survival rate related to preterm birth • still-births are generally not included Stefan Johansson
Why preterm deliveries? induced spontaneous Stefan Johansson
Induced preterm delivery • Preeclampsia (hypertension and urinary protein leakege) • delivery on ”maternal indication” • delivery on ”neonatal indication” • Other indications • maternal diseases (diabetes, cancer, trauma etc, etc) • fetal growth retardation • multiple pregnancies • malformations Stefan Johansson
Spontaneous preterm delivery • Infections (malaria) • Preterm rupture of membranes (PROM) • Preterm contractions • Placental bleeding Stefan Johansson
Risks of recurrent preterm delivery Ananth. AJOG 2006;195:643 Stefan Johansson
Risks of recurrent preterm delivery, 34-36 wks Ananth. AJOG 2006;195:643 Stefan Johansson
Risks of recurrent preterm delivery, < 28 wks Ananth. AJOG 2006;195:643 Stefan Johansson
Preterm birth… genes or environment? Stefan Johansson
Risk factors of preterm birth - genes • Genetic influence on gestational length. • genetic factors accounted for 36% of preterm births • Genetic component of pre-eclampsia • heritability for preeclampsia was 31% • If the mother/sister had preeclampsia, the risk of preeclampsia for the daughter/sister is tripled, compared to unrelated women. Clausson. BJOG 2000;107:375 Nilsson. BJOG 2004;111:200 Stefan Johansson
Risk factors of preterm birth - infections • Reproductive tract infections* have increased risk • 20% of women with infections delivered preterm compared 9.5% of women without infection. • More than 40% of preterm deliveries attributed to infections. • Treatment of infections reduced the risk of preterm delivery • Relative risk 0.16 [0.04-0.66] French. AJOG 2006;194:1717 *bacterial vaginosis, Chlamydia, Trichomonas, Mycoplasma, gr B strepto, Gonorrhoeae Stefan Johansson
Risk factors of preterm birth - maternal age • Young maternal age • Teenage women have a doubled risk of preterm birth,compared to women aged 20-24 • High maternal age • Women aged ≥40 are also at increased risk of preterm birth Olausson. BJOG 2001;108:721 Cleary-Goldman, Obstet Gynecol 2005;105:983 Stefan Johansson
Risk factors of preterm birth - education Thompson. Paediatr Perinat Epidemiol. 2006;20:182 Stefan Johansson
Risk factors of preterm birth - smoking Kyrklund-Blomberg. AJOG 1998;179:1051 Stefan Johansson
Risk factors of preterm birth - others • Periodontal infections. • Interpregnancy weight loss. • Previous induced abortion. • Air pollutants and ozone. Stefan Johansson
Increasing rate of preterm birth - what to do? • Reduce the prevalance of smoking? • Screen for bacterial vaginos, chlamydia and other infections? • Sharpen indications for induced preterm deliveries? • More knowledge is needed aboutmodifiable risk factors. Stefan Johansson
Conclusions • Preterm birth is common and rates are increasing. • Substantial mortality. • Methodoligical issues. • Many risk factors identified: • genes • Infections • maternal age • Socioeconomic status • smoking • No succesful strategies to prevent preterm birth. Stefan Johansson