Download
1 / 39
390 likes | 405 Views
Learn about the design and implementation of a fast track service for the diagnosis and management of Malignant Spinal Cord Compression (MSCC). Understand the effects of MSCC, who is at risk, and the importance of early diagnosis. Discover the symptoms of MSCC and the management steps once it has occurred.

E N D
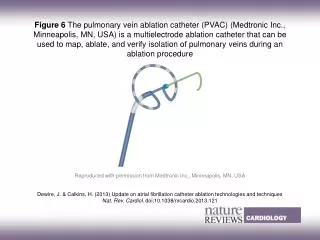
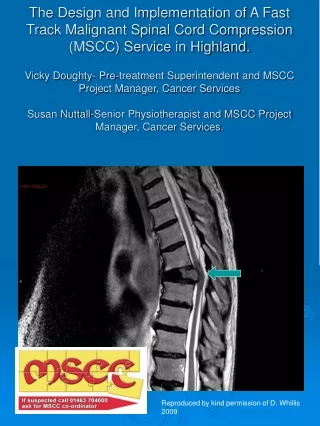
The Design and Implementation of A Fast Track Malignant Spinal Cord Compression (MSCC) Service in Highland.Vicky Doughty- Pre-treatment Superintendent and MSCC Project Manager, Cancer ServicesSusan Nuttall-Senior Physiotherapist and MSCC Project Manager, Cancer Services. Reproduced by kind permission of D. Whillis 2009
What is Malignant Spinal Cord Compression (MSCC)? “Spinal cord or Cauda equina compression by direct pressure and/or induction of vertebral collapse or instability by metastatic spread or direct extension of malignancy that threatens or causes neurological disability. Nice Clinical Guideline 75 Metastatic Spinal Cord Compression November 2008
What are the effects of MSCC? Paralysis from the level of the compression, if presentation is late.
Who is ‘at risk’ and incidence? • Early diagnosis is a priority (Evidence base) • Management once MSCC has occurred (Evidence base) • Progress re implementation
Who is at risk? • Stats:- General incidence 5-10% of patients with cancer will develop MSCC, (3-7.4% of all patients with Ca lung, breast and prostate) • Professionally: GP’s would rate the condition as rare (2-3 in GP Career) Oncology Consultants - quite common, Palliative Medics – common++, • Other statistics estimate that 75% of MSCC go undiagnosed, (diagnosis made at post-mortem) clinical presentation is of an elderly patient with a cancer Hx who has gone off their feet.
MSCC Facts • Commonest cause is blood spread (85%) • Less common is direct invasion or direct deposition of tumour cells. • Compression causes Oedema, Venous Congestion and demyelination. • If gradual, effects can be reversible. • Prolonged compression causes vascular injury resulting in Cord Infarction, this is not reversible.
MSCC Facts • T spine is commonest site (68%) • The site of pain is not always the site of the compression • 54% pts with upper T Spine compression had Lumbar pain • Sensory level does not always correspond with site of compression (could be out by many dermatomes) useful in only 16% of cases • Sensory level is a late indicator of cord compression
Early diagnosis is a priority • Refs:- Clinical Research and Audit Group Report, 2001 • Levak et al, Clinical Oncology, 2002, 14, 472-480
What the CRAG report found:- Time line of events leading to MSCC 1st Symptomtells GP referredDx Patient 3 wks GP + hospital system 9 weeks --------3 months-------- Back Pain Neurogenic pain - 2 months 3 weeks
FACT • If a patient presents with paraplegia due to MSCC it is unlikely that they will walk again. • The Scottish Executive Clinical Research and Audit Group study in 2001, found that 48% of their study population were unable to walk at diagnosis.
Is it clinically possible to determine the level of compression without Ix? NO!!!!!!!!!!! Pain felt is unlikely to be were the site of compression is. Graphs:- site of pain / site of compression root pain / level of compression sensory level / level of compression All graphs mis-match.
The definitive test for diagnosis of MSCC Is a whole spine MRI scan CRAG Audit Results showed less than 1 in 5 plain films, and less than 1 in 5 bone scans were predictive of MSCC. Also that when x-rays were taken, most x-rays were of the lumbar spine and most of the compressions were at thoracic level.
What has developed from the CRAG report? A clinician, Dr Pam Levak, spearheaded a campaign entitled ‘QED’ QUERY EPIDURAL DISEASE It took her at least 3 years but she finally realised her dream and developed a QED Hotline in Dundee in 2004. Sept 2005 Update:-In Tayside the Hotline was a victim of its own success. It was so successful that it is now no longer required as a special service, it has become “Best Practice”
What are we looking for ? Pt with known history of cancer especially lung, breast, prostate, Lymphoma and Multiple Myeloma. Who presents with new back pain, which is worse on lying down, radicular, worse on coughing, night pain.
MSCC Symptoms • Localised Back Pain (Progressive and latterly Severe) Sharp, Shooting, Burning are common descriptors. • Nerve Root pain (Like a band around chest or sore frontof thighs). • Weakness in one or both legs. May be reporting unexplained falls. • Neuro Symptoms. (Numb/Tingling/Proprioception) • Problems passing urine/faeces. (Think of Opioids) • Paralysis
Dr Levak says … • It is not clever to diagnose MSCC once someone has gone off their feet!!! • Weakness is a late sign so don’t wait for it to happen!!!!!
Message? Query Epidural Disease
Step 2 Management once MSCC has occurred:- Pease, Harris and Finlay (2004) “Development and audit of a care pathway for the management of patients with suspected Malignant Spinal Cord Compression” Physiotherapy, Vol 90, No 1, Pp27 – 34. Provides the evidence base.
STABLE OR UNSTABLE? WE NEED TO KNOW!
Design and Implementation of a Fast Track Malignant Spinal Cord Compression Service
The Spinal Cord…a little revision! A Cylindrical structure constituting the central nervous system, extending from the Medulla to the lower border of L1 where it then becomes the Cauda Equina or the horses tail. It is surrounded by the 3 layers called the meninges and bathed in Cerebrospinal Fluid or CSF. There are 31 pairs of spinal nerves 8 Cervical, 12 Thoracic, 5 Lumbar, 5 sacral and 1 Coccygeal. This constitutes the peripheral nervous system. Reproduced by kind permission of S.Garrett 2009 Function: allows nerve impulses to travel between brain and body
MSCC-in many forms. Most commonest form is Epidural tumour causing vertebral collapse. Leptomenigeal deposits are found within the 2 inner layers. Harder to diagnose. Show up as a bright thickening on MRI. Intramedullary arise within the cord. Associated with drop Mets i.e. Intercranial disease
So Why Implement a Fast Track MSCC Service? • Patients Perspective • Referrers Perspective • Hospital Perspective • Nice Guidelines Nov 2008 Our existing ‘pathway’ was non existent! With ‘some’ work this is what we came up with!!!
REFERRAL “Can you bleep the Malignant Cord Compression Team” TRIAGE TEAM Bleep xxxx 9am to 5pm 5pm to 9am MDT TRIAGE TEAM TRIAGE QUESTIONS D/W CONS ONC CONS/ONC ON CALL ASKS QUESTIONS NO YES CO-ORDINATION OF MDT PHYSIO/OT (blp1184) CONS ONCOLOGIST MRI SCANNER (6050) SIMULATOR (4581) LINAC (TREATMENT)(5897) WARD 2C (5793) CONTACT REFERRER CONTACT REFERRER TO OFFER ADVICE CLINICAL STABLE/UNSTABLE REQUEST MRI PROV REQUEST RADIOTHERAPY ADMISSION CT (If no MRI) MRI SCAN CLIN ONC TO INFORM DUTY HOUSE OFFICER BLEEP TRIAGE WITH RESULTS Bleep XXXX -VE +VE PAIN FUNCTION PROBLEMS METASTATIC DECISION TO TREAT BACK TO CLIN ONC IF NO REQUEST FOR RADIOTHERAPY CONSENT BACK TO REFERRER RADIOTHERAPY DOCUMENTATION URGENT RADIOTHERAPY SIMULATE SPINE BLEEP PHYSIO (1184) NEURO SURGICAL OPINION ADMIT YES NO STABLE/UNSTABLE RADIO- THERAPY KEEP WALKING AS ABLE LOGROLL PRECAUTION BED MANAGER or OTHER ONGOING CARE BRACE + REHAB SURGERY + REHAB
Reasons for implementation • Existing pathway involved multiple disciplines (Largely unaware of each other)! • It lacked co-ordination, structure and understanding of each disciplines role in MSCC. • Lack of coherence. • Conflicting information given to patients/staff which resulted in delays in diagnosis and treatment/rehabilitation.
Patients Perspective Early Onset + Early treatment = Better QOL Improved Mobility Maintained Independence Late Treatment= None of the above and increased complication and mortality rate.
Referrers Perspective. • Clear, efficient and streamlined referral pathway. • Timely referral to correct services. • Advice, support and feedback via Triage Team • Assurance that patient will follow a consistent pathway to treatment.
NHS Perspective • Our objective was always to redirect resources into patient focused care. • Reduce inefficiency and create a better system of work. • Using a successful template from Tayside, tailored to meet the specific demands of Highland, structure a pathway of our own.
Our Approach 2 Project Managers (Clinically Based) Stakeholders GP, Physio (rehab), Radiotherapy, Radiology (MRI), Oncologist Regular updates and feedback Triage Team Nurses, Radiographers (T), Physiotherapist, Occupational Therapist Implement/launch/triage duties
Our Approach Health Professionals (community) Palliative care (community) Outpatient Depts Oncology Dept awareness sessions Wards GP practices Peripheral Hospitals Start small and local to check infra structure. Once out in the ‘public domain’ its hard to control
Our Approach to Training • Triage Training 5 Staff members operating a rota system. In house Triage Training in liasion with Oncology Consultants. In depth scenario training using actual case studies with feedback from Oncology Consultants. Standardised documentation. Audit under development Why have a logo? It gives us an identity and ownership. The puzzle is a visual prompt.
The MSCC Co-ordinator Role • Voluntary Rota (alongside daily clinical duties) • On call from 9am til 5pm Mon-Fri (then covered by on-call oncologist out of Hours. • Liaises directly with on-call oncologist regarding triage/management. • Co-ordinates admission/MRI/Simulation and Radiotherapy/PT and OT.
The MSCC Co-ordinator Role….what the referrer would expect. • Timely response and explanation of process. • Taken through a series of triage questions • A named point of contact. • Advice and feedback. • Logical approach to transfer of patient to appropriate services.
Malignant Spinal Cord Compression Triage Questions. Question Indicator What makes you suspect this is Malignant Spinal Cord Compression? Is there a history of Cancer? Or Is the patient under Investigation for Suspected Cancer? Common Cancer types inc:- Lung, Breast, Prostate, Myeloma and Lymphoma Is the patient complaining of new or worsening pain? What is the site of the pain? Ant Thigh pain, Radicular pain (like a band), Stopping pt from sleeping? Must be new difficulty, could include weakening in legs. Is there any reported new difficulty walking? Is there any reported neurological symptoms? Bladder/Bowel incontinence. Altered sensations, numbness/tingling. Proprioception (awareness of difficulty in placing their feet) Is the patient suitable for MRI? Refer to MRI Safety Checklist (located in MSCC Folder)
IMPORTANT What you need to know • If You Suspect MSCC speak to someone. • Anyone can bleep the MSCC Co-ordinator. • Use the correct Phraseology at switchboard. • ‘Malignant Spinal Cord Co-ordinator’ • If it doesn’t fit our pathway we will tell you and advise on an alternative route.
Results at 6 months • Number of referrals = 25 • Number of positive cords = 8 • No of Cauda Equina = 6 • No of patients scanned/not Rx = 5 (2 allowed significant subsequent diagnosis to be made) • Not Scanned = 2(seen by consultant) • No inappropriate referrals = 4
References P.Levak et al. Don’t wait for a sensory level – Listen to the symptoms: a prospective Audit of the Delays in Diagnosis of Malignant Cord Compression. Clin Oncol 2002:14:472-480 Metastatic Spinal Cord Compression: Diagnosis and Management of Patients at risk of or with Metastatic Spinal Cord compression. Nice Clinical Guidelines Nov 2008 L Allan et al, Suspected Malignant Spinal Cord Compression – improving time to diagnosis via a ‘hotline’: a prospective audit. British Journal of Cancer 2009, 100, 1867 -1872.