SARS Outbreak in Hong Kong
430 likes | 604 Views
SARS Outbreak in Hong Kong. Professor Peter Cameron Previously COS Prince of Wales Hospital Chinese University of Hong Kong. Background. Aware of Reports of Atypical Pneumonia in Guangzhou Reported 305 cases and 5 deaths and then information ceased Thought that it was probably worse

SARS Outbreak in Hong Kong
E N D
Presentation Transcript
SARS Outbreak in Hong Kong Professor Peter Cameron Previously COS Prince of Wales Hospital Chinese University of Hong Kong
Background • Aware of Reports of Atypical Pneumonia in Guangzhou • Reported 305 cases and 5 deaths and then information ceased • Thought that it was probably worse • ? Chlamydia • A couple of unusual cases admitted to HK hospitals – died, no secondary spread
Index Case Prince of Wales • Admitted Ward 8A, March 4, 2003 • 26 yo ethnic Chinese, symptoms of high fever, myalgia, and cough • One ED attendance 4 days previously for fever and myalgia • Diagnosed with pneumonia and treated with augmentin and clarithromycin • Improved over one week • No unusual features
Recognition of Outbreak • Staff of 8A noticed a number of medical and Nursing staff sick • ? Influenza – Discussion regarding isolation • Area with separate ventilation, entry from main wards • ? ED Observation Ward • Discussion with CEO, Prof Medicine and ED • Establish Facts • 15 medical and 15 Nursing staff sick • 5 ED docs and 3 nurses • Other pts and visitors • Medical students
Response • Symptomatic staff isolated to ED Observation Ward • Not all staff complied • ?over reacting • CEO called council of war next morning of service chiefs – then twice daily • Hospital continued normal services initially • 2-3 days to recognise internally the extent of the problem
Response • Community aware that PWH had a problem within 2 days • Thought to be internal and government supported this view • Did not ban visitors initially • Balance between panic/service/managing an outbreak
Unknown • Nature of organism • Mode of spread • Extent of spread • Outcome • Likely epidemiology • ?world pandemic
Quarantine • Intense lobbying by senior clinicians • Staff afraid to go home at night • Visitors • Patients • Elective • Specialist • Emergency • Possible cases • Home vs ward isolation • Screening procedures
Reported Clinical Features(Inpatients) • Incubation period – 2-7 days but ?16 days • Symptoms • Fever 100% • Chills/rigors 73.2% • Myalgia 61% • Cough 57% • Headache 56% • Dizziness 43% • Also N&V, diarrhea, abdo pain, coryza, sore thoat ~20%
Initial Symptoms at a Screening Clinic SARS - SARS+ • Fever 37% 81% • Chills 21% 52% • Malaise 20% 34% • Myalgia 12% 27% • Rigor 4% 12% • Cough 72% 64% • URI neg predictor • LOA/Vomiting/Diarrhoea Pos Predictors
Epidemiology • Contact tracing • Health department processes not adequate • Expertise?
Infection control • Droplet spread • Mask, glove, cap and gown • Surfaces/fomites • Hood/visor for procedures • Viral filters • Other modes of spread? • Definite evidence of faecal/urine viral loads • No evidence of airborne – negative pressure unnecessary
Airborne Spread • Nebulisers • Non Invasive Ventilation • Continuum between aerosol and droplet
Engineering • Ventilation • Toilet layout • Sewage • Negative pressure rooms • Ward layouts
Treatment • Empiric treatment • Antivirals - ribavirin • Steroids • Cytokine inhibitors • Convalescent serum • Traditional chinese medicine • Ethics? • Political pressure
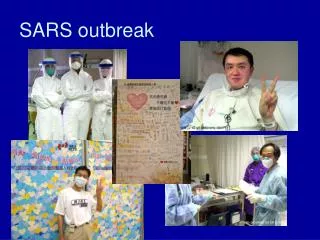
Staff Morale • Service chiefs – daily updates • Staff forum daily • Web site updates • Daily ward round by senior staff • CEO of hospital and Hospital Authority contracted disease • Face to face meetings – danger of cross infection • HKSAR CEO perceived badly for not being on site
Families • Important aspect of staff morale • Should staff stay in quarters – increased risk for staff • Isolation of staff from families • Possibility of months • Send family away – increased risk to other communities • If staff go home – what precautions needed?
Outcomes in PWH • 20-30% of all pts in ICU • No nursing or medical staff at PWH died • >100 staff and med students affected • Initial mortality ~5% but case fatality rate >10% • In elderly >50% • Long Term? • Pulmonary fibrosis
Outcomes in HK • ~ 1700 cases • ~300 deaths • Outbreak over in less than 3 months • ~25% cases staff
Community Response • Hospitals • Initially PWH • Other hospitals became involved • Infectious disease hospital • Overloaded
Community Response • schools • Tourist and economy • Goverment
Microbiology • Uncertainty about organism • Tests actually caused problems • Not properly trialled for accuracy
Serologic confirmation of cases • Coronavirus confirmed in virtually all those with classic course • Very few cases with no symptoms and CoV serology • Reason for immunity? • Mucosal barrier • IgA
Lessons Learnt • Politics of Infectious disease ugly • Little is known about infectious disease • Basic infection control works • Basic Infection control is not done well • Hospital workers are at risk • Authorities are always behind in managing disasters • Don’t try to predict nature • Life Returns to normal quickly