Download
1 / 60
620 likes | 1.08k Views
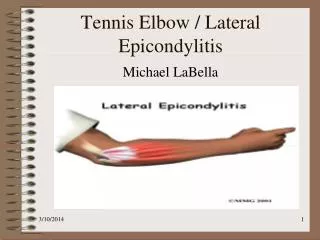
TENNIS ELBOW An 2012 Update. Prof. Dr. Khalid Idris Professor of Orthopedic Surgery, Faculty of Medicine, Zagazig University EGYPT. Tennis elbow refers to a syndrome of pain centered over the common origin of the extensor muscles of the fingers and wrist at the lateral epicondyle.

E N D
TENNISELBOWAn 2012 Update Prof. Dr. Khalid Idris Professor of Orthopedic Surgery, Faculty of Medicine, Zagazig University EGYPT
Tennis elbow refers to a syndrome of pain centered over the common origin of the extensor muscles of the fingers and wrist at the lateral epicondyle. • It affects 1% to 3% of adults each year.
It was first reported in the literature in 1873 by Runge . It occurs more commonly in non-athletes than athletes and has a peak incidence in the fifth decade.
It may be caused by repeated microtrauma to the origin of extensor carpiradialisbrevis (ECRB) but the precise etiology is still unclear. Collateral ligamentouscomplex ,joint capsule and synovitis (with or without plica) also have been implicated.
Sources of Pain • The etiology of pain generation in tennis elbow is multifactorial. • It is likely that both intra- and extra-articular structures produce symptoms and that the contribution of each varies between patients.
Regan et al in 1992 demonstrated that the initial lesion of ECRB is a hypoxic degenerative process (rather than inflammatory) that can be a normal part of aging or the response to stress of overload and overuse.
An incomplete healing response characterized by vascular and fibrous proliferation occurs in the area of poor vascularity.
This may well represent the ‘‘angiofibroblastic hyperplasia’’ coined by Nirschl (1994) to describe the pathological invasion of blood vessels, fibroblasts, and lymphatics into the symptomatic area of the extensor carpi radialis brevis.
As the degenerated areas enlarge, the tendon weakens and eventually ruptures (microrupture), which initiates the classic inflammatory response and healing cascade, explaining spontaneous recovery in some cases.
Arthroscopic Classification Type I lesions appeared arthroscopically with intact capsules; Type II were linear tears at the undersurface of the capsule; and Type III were complete tears of the capsule with partial or complete avulsions of the ECRB tendon (Dlabach and Baker, 2001).
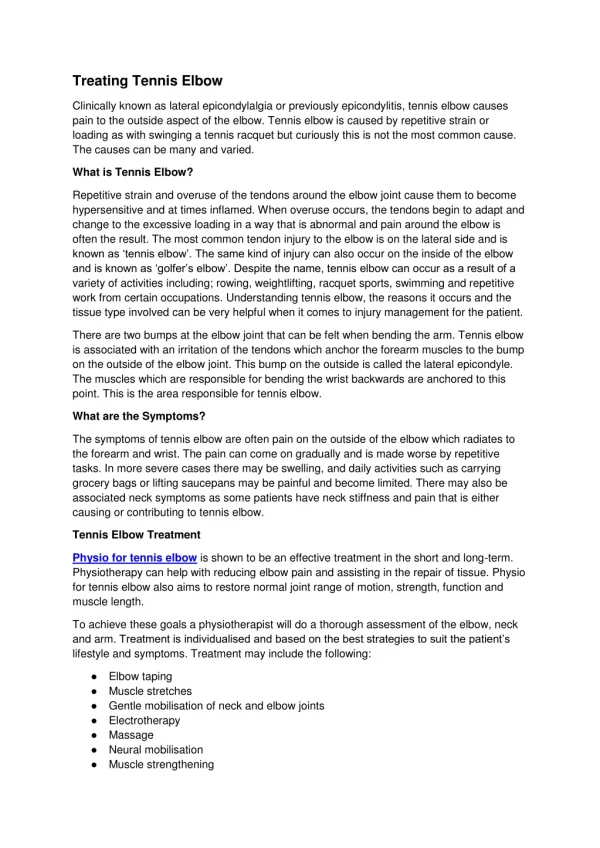
DIAGNOSIS **Localized discomfort to the origin of ECRB **Tenderness over the lateral epicondyle approximately 5 mm distal and anterior to its midpoint. **Pain usually is exacerbated by resisted wrist dorsiflexion and forearm supination, **pain when grasping objects.
Plain roentgenograms usually are negative; Occasionally calcific tendinitis may be present. MRI demonstrates tendon thickening with increased T1 and T2 signals but generally is not indicated.
DIFFERENTIAL DIAGNOSIS ##Osteochondritis dissecans of the capitellum ##Lateral compartment arthrosis, ##Varus instability, and perhaps most commonly, ## Radial tunnel syndrome.
The pain of radial tunnel syndrome is located 3 to 4 cm distal to the lateral epicondyle and may be reproduced with long finger extension against resistance. The latter finding is inconsistent, as are abnormalities on EMG. True tennis elbow and radial tunnel syndrome may coexist in up to 5% of patients.
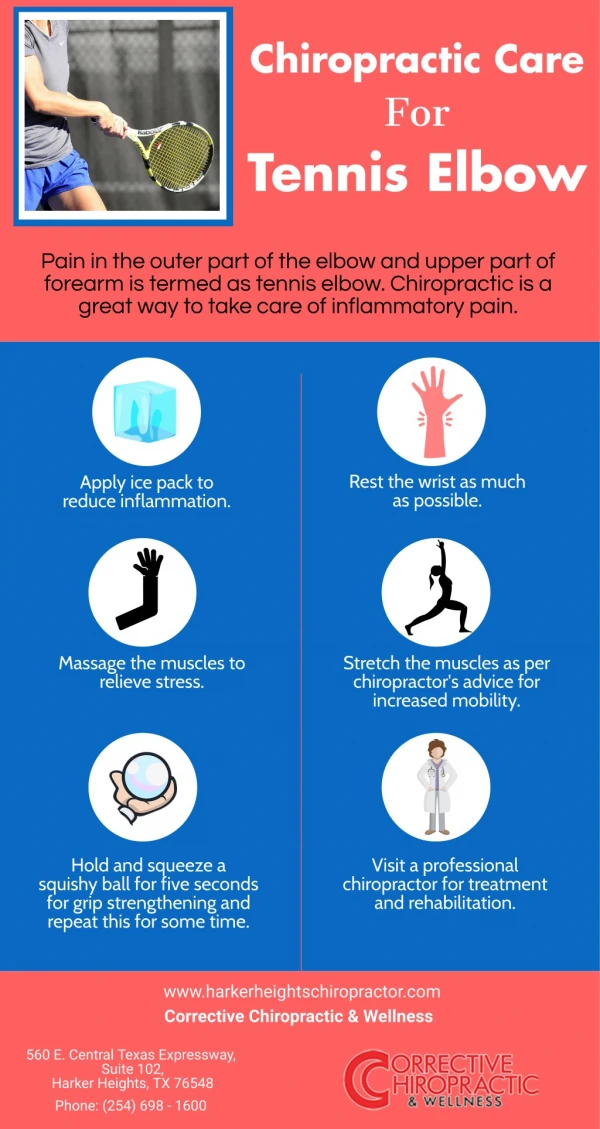
NONOPERATIVE TREATMENT Rest, ice, oral and topical NSAIDS, Steroid injections (not through the tendon!!). Physical therapy such as ultrasound, iontophoresis, electrical stimulation, manipulation, soft tissue mobilization, friction massage, stretching and strengthening (especially eccenteric) exercises.
Bracing • Proximal forearm band . • Cock-up wrist splint.
NONOPERATIVE TREATMENT As an adjunct to local injection an attempt to "complete the lesion" by forcibly flexing the wrist after local anesthetic injection to initiate the inflammatory cascade and induce healing can be done.
NONOPERATIVE TREATMENT Preliminary data from studies reporting newer treatment methods such as low-level laser and extracorporeal shockwave therapy are promising, but further investigation is necessary.
Botulinum toxin, a presynaptic acetylcholine blocker, has recently been proposed as a treatment. The reported mechanism is partial paralysis of the extensor apparatus, which allows the tendinous origin to heal in a less tensioned environment.
Other Modalities • Noncoherent light, which is thought to act via improving local blood supply, • Topical nitric oxide, iontophoretic dexamethasone, and autologous blood injection.
OPERATIVE TREATMENT The vast majority of cases usually resolve with conservative treatment. Those who fail to respond may require surgery. Most studies reported that 5– 10% of patients require surgery.
OPERATIVE TREATMENT Operative treatment is considered if prolonged (6 to 12 months) nonoperative treatment is ineffective. Surgery is effective in 90% of properly selected patients.
The operative procedures that have been described for tennis elbow may be divided into six groups:
The first and most frequently used procedure is a release of the common origin of the extensors by division of the origin at the lateral epicondyle either with an open procedure or with a percutaneous technique or lengthening of ECRB to decrease the tensile forces on the extensor origin .
In the second type of procedure, the area of the rupture of the extensor origin is excised, creating a longitudinal defect in the origin, which is repaired by suturing.
The third procedure, which was used by Kaplan {1959} and by Wilhelm and Gieseler {1962}, is operative denervation of the lateral epicondyle. This is accomplished by severing of the sensory fibers of the radial nerve that innervate the lateral epicondyle.
The fourth group comprises several types of intra-articular procedures including partial or complete division of the annular ligament, synovectomy, with or without debridement of an osteoarthrotic radial head and these procedures are combined with release of the extensor origin.
The fifth type of operative treatment is a release of the posterior interosseous nerve from the radial tunnel, combined with division of the fibrous edge of the superficial portion of the supinator muscle (the arcade of Frohse).
The sixth and most recent group comprises arthroscopic procedures. Arthroscopy allows intraarticular examination for other pathology and permits a shorter postoperative rehabilitation period and an earlier return to work.
Surgical technique for correction of tennis elbow. A, Skin incision. B, Origins of extensor carpiradialislongus and extensor digitorumcommunis are identified. C, Osteotomedecortication. (Redrawn from Nirschl RP, Pettrone F: J Bone Joint Surg 61-A:832, 1979.)
Surgery for tennis elbow (Boyd and McLeod). A, Approach and incision. B, Reflection of conjoined extensor tendon, excision of proximal 2 mm of annular ligament, and removal of strip of capsule containing synovial fold from radiohumeral joint. (Redrawn from Boyd HB, McLeod AC Jr: J Bone Joint Surg 55-A:1183, 1973.)
Anconeus muscle transfer. A,B, Entire common extensor origin is excised C, Anconeus muscle rotated into defect (Redrawn from Almquist EE, Necking L, Bach AW: J Hand Surg 23A:723, 1998).