Download
1 / 43
430 likes | 684 Views
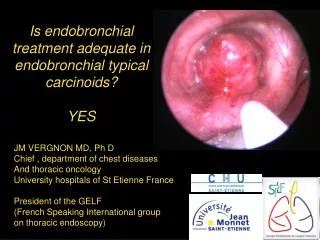
ENDOBRONCHIAL TREATMENT MODALITIES HOT PROCEDURES Dr. Murat SEZER MD, Assoc.Prof. I declare that I have no conflict of interest with any company. Mali gnant Airway Obstruction. At initial admission 80% of lung cancer patients are inoperable, and are candidates for palliative therapies.

E N D
ENDOBRONCHIAL TREATMENT MODALITIES HOT PROCEDURES Dr. Murat SEZER MD, Assoc.Prof.
I declare that I have no conflict of interest with any company.
Malignant Airway Obstruction • At initial admission 80% of lung cancer patients are inoperable, and are candidates for palliative therapies. • At the time of diagnosis 50% of lung cancer patients have malignant airway obstruction. • Belani CP. Multimodality management of regionally advanced non-small-cell lung cancer. Seminars of Oncology 1993; 20: 302 • Herth FJ, Eberhardt R, Vilmann P, et al. Real-time endobronchial ultrasound guided transbronchial needle aspiration for sampling mediastinal lymph nodes. Thorax 2006;61:795-8.
Malignant Airway Obstruction • Endotracheal or endobronchial obstruction due to malignant disease causes: • Cough • Shortness of breath • Obstructive pneumonia • Endobronchial treatment improves; • Symptoms and • Quality of life
Malignant Airway Obstruction • Procedures with rigid bronchoscope under general anesthesia allows • Maintainance of adequate ventilation, • Removal of larger volumes of tumour, • Safely control of larger amounts of hemorrhage
Advanced Stage Lung Cancer Laser APC Electrocautery Brachitherapy Cryotherapy PDT Stent placement + 0 ++ ++ 0 ++ 0 +++ ++ . endoluminal extraluminal mixed
Laser Bronchoscopy • Light • Amplification (by) • Stimulated • Emission (of) • Radiation Intense light radiation Heat Tissue damage
Laser Wave Length and Advantages • Nd-YAG Laser Coagulation (1064 nm) Deep penetration Vaporisation • KTP (532 nm) Deep coagulation Precise excision • Argon beam (488 nm) Coagulation • Diode (810 nm) Coagulation Cutting
Characteristics of Nd-YAG laser • Well absorbed by pigmented tissues • Excellent photocoagulation • Thermal damage to adjacent tissues • Invisible (infrared range, guidelight) • Deep penetration possible
Personnel • Should have expertize both in flexible and rigid bronchoscopy • Working knowledge of laser physics • Accreditation by an institution’s laser committee may be required • In addition to required personnel for standard bronchoscopy, one assistant should have sole responsibility for controlling the laser • Protective eyewear is required for the patient as well as the laser team
Technique • Laser bronchoscopy can be performed with flexible or rigid bronchoscopes • To minimize the risk of hemorrhage it is important to coagulate the lesion with low laser power before resection • Laser fibre tip should be at least 3 mm from the target tissue to avoid the tissue being vaporised
Technique • Continuous suction is used during the procedure to remove smoke from the airways • Continuous inspection of non-obstructed airways is performed to remove any debris and to optimize ventilation • Inspired oxygen is limited to 40% to reduce the risk of airway fire • Laser exposure should be kept to a minimum
Indications • Immediate relief of endobronchial obstruction due to primary lung cancer or metastatic disease • Central or segmental airway strictures or scarring Tbc Inhalation injury Prior lung resection Endotracheal intubation Trauma Previous laser surgery Radiation therapy Foreign body obstruction Tracheotomy, tracheostomy
Contraindications • Tracheoesophageal fistula • Uncorrected coagulopathy • Total airway obstruction with little if any functional distal airway open • Little or no exophytic lesion visible
Complications • Massive hemorrhage • Pneumothorax • Pneumomediastinum • Procedural death rate %2-3 • More airway scarring and subepithelial fibrosis than other immediate debulking techniques • Hipoxemia • Perforation and fistulae formation • Fire in the airway
Electrocautery • Application of a high frequency electrical current to coagulate (lower temperatures) or to vaporise tissue (higher temperatures) • The current is delivered endobronchially via a probe, snare or needle knife. • A monopolar technique is used in the airways • The degree of tissue destruction depends on: The power used Duration of contact Surface area of contact Density and moisture content of the tissue
Equipment • High-frequency electrical generator • Insulated probe • A neutral plate to complete the circuit • An insulated instrument to prevent electrical current leakage, if the procedure is performed with a flexible bronchoscope
Technique • The passage of an uncuffed endotracheal tube over the flexible bronchoscope at the beginning of the procedure can facilitate repeated removal of resected tissue • The initial energy setting (around 20W) should be tested on normal mucosa before treating the lesion • Duration of the treatment will affect the depth of tissue damage (30W in 1 sec: 0.1 mm 5 sec: 1.9mm) • Longer duration of coagulation (3-5 s) causes damage to underlying cartilage • It is necessary to continuously remove mucus, debris and blood to avoid current leakage
Technique • The Probe may be used to vaporise superficial tumours • The Snare is useful for debulking large volumes, especially polypoid tumours • The Knife is particularly useful for resecting benign webs • Removal of large volume tumour from the airway can be achieved in a variety of ways: • Suction • Grasping or biopsy forceps • Use of a cryoprobe
Indications • Similar indications with laser bronchoscopy • The prospective management of benign stenoses using electrocautery is effective • Removal of granulation tissue • Removal with curative intent of both benign and early stage malignant tumours
Contraindications • Presence of a pacemaker susceptible to electrical interference • Exclusive extraluminal obstruction of the airway • A relative contraindication is the presence of a metallic object in the close proximity to either electrode
Complications • Bleeding • Airway fire • Careful application of the patient plate and the use of insulated bronchoscopes reduce the risk of current leakage causing burns • It is recommended that the skin surface overlying a metallic joint prothesis be avoided when placing return electrodes for electrocautery
Argon Plasma Coagulation • APC is a non-contact mode of electrocautery • Argon gas is used as the conductive medium • It causes desiccation and coagulation of exophytic endobronchial tumors • It can provide rapid haemostasis when used to treat haemoptysis arising from visible endobronchial lesions
Equipment In addition to the equipment required for electrocautery: • Argon gas (a tank with a flow meter) • A microelectrode catheter to transport gas and electrical current simultaneously
Technique • APC does not make contact with the tissues it destroys and has a penetration depth of just a few millimeters • It is more suitable for the treatment of superficial and spreading lesions • Once gas is released through the catheter tip, it is ignited through electrical current • An arc is formed if the probe is close enough to the mucosal surface, causing heat destruction and desiccation of the tissue • The arc can be moved back and forth (painting)
A: Desiccation B: Coagulation C: Devitalization
Indications • The treatment of haemoptysis caused by lesions within the central airways • Debulking of exophytic endobronchial tumours, both benign and malignant • Debulking of granulation tissue arising as a complication of tracheobronchial stent insertion
Contraindications • For lesions causing significant tracheal obstruction rigid bronchoscope should be used instead of flexible bronchoscope or the latter one can be used with endotracheal intubation • APC is contraindicated where there is a requirement for a FiO2 >40% because of the theoretical risk of endobronchial fire • Most modern implantable cardiac pacemakers or defibrillators are compatible with electrocautery and APC, but advice should be sought from the patient’s cardiologist prior to the procedure
Complications • Reichle et al reported bronchial or tracheal perforations in 5/364 patients, all of which resolved on treatment • Three patients developed temporary post-procedural neurological complications • Two patients died (myocardial infarction, hypovolemic shock) • The neurological and cardiac complications in these 5 patients may have been caused by intracardiac gas embolism • Reddy et al also reported 3 cases of intracardiac gas embolism (2 fatal) • All were treated using rigid bronchoscopy and it is not clear whether gas embolism arose as a complication of APC or of jet ventilation
Bronchial Thermoplasty • The goal is to reduce airway smooth muscle • The treatment is performed via flexible bronchoscopy under conscious sedation • Microwave energy is delivered to the bronchial wall via a flexible catheter from a radiofrequency generator • This heats the airway wall to about 65oC and selectively ablates the concentric smooth muscle • The airways are treated in a systematic manner from distal to proximal • The right lower lobe is treated first followed by the left lower lobe 3 weeks later, then the upper lobes
Indications • Thermoplasty may be indicated in patients with severe persistent asthma receiving high-dose combination inhalers (>1000 µg beclometasone equivalent) plus long-acting bronchodilators or long-term oral corticosteroids. • The FEV1 should be >50% predicted
Complications • Patients may experience post-procedure respiratory exacerbations • Limited long-term safety data for this procedure are available