Download

1 / 76
840 likes | 1.12k Views
Bariatric Surgery Center of Excellence Site Inspection Process. Judy Crouch, RN, MSN,, APRN, BC, CBN Senior Site Inspector Michigan Bariatric Society 2 nd Annual Meeting Friday, November 13, 2009.

E N D
Bariatric Surgery Center of Excellence Site Inspection Process Judy Crouch, RN, MSN,, APRN, BC, CBN Senior Site Inspector Michigan Bariatric Society 2nd Annual Meeting Friday, November 13, 2009
“Quality is never an accident; it is always the result of high intention, sincere effort, intelligent direction and skillful execution. It represents the wise choice of many alternatives.” William A. Foster
What is excellence? Gold standard Sterling #1 Outstanding Distinguished Firstclass Exceptional Remarkable Extraordinary Superior
Surgical Review Corporation (SRC) Mission Statement Surgical Review Corporation assesses and improves the efficacy, efficiency and safety of surgical and related health care.
Why have Bariatric Surgery Centers of Excellence? • Establish criteria for assessing bariatric surgical practices • Evaluate applicants to ensure they meet established standards • Collect, analyze and disseminate data • The opportunity for applicants: • Access to support by SRC’s staff • Site inspection process offers opportunity to find strengths and weaknesses in program structure • Objective review by experienced bariatric surgeons
The Trinity Hospital Surgeon Practice
Application & Approval Process • Provisional application and approval • Full application • Site Inspection • Submission of site inspection data • BSRC review process • ASMBS Executive Council • Contract signed and returned to SRC • CMS notified and center is added to SRC website
Role of the Site Inspector • Gather objective data • Observe • Document compliance with the 10 Requirements • Act as the eyes and ears of the Bariatric Surgery Review Committee (BSRC) • Does NOT offer subjective opinions or personal recommendations to the BSRC
The Bariatric Surgery Review Committee (BSRC) • Consists exclusively of experienced, respected bariatric surgeons • Members are from all geographical areas of the country • There is a mix of private practice surgeons and surgeons from academic practice • Appointed for three-year terms • Role is to review the data submitted for Provisional Status, Full Approval application and the site inspection and to make recommendation for approval or denial. • Clarifies existing requirements and makes recommendations for revisions of existing requirements to the SRC Board of Directors
SRC Support System SRC is committed to helping applicants thoroughly prepare for a successful site inspection. • A pre-site inspection letter and checklist detail the site inspection process and the documents needed for review during the site inspection. • Site inspectors are available prior to the site inspection to answer questions. • SRC Support Center: 866.790.4772 srcsupport@surgicalreview.org • Site Inspectors host a weekly teleconference “Ask SRC” every Monday from 12 – 1 PM EST. • Judy.crouch@surgicalreview.org
For More Information: www.surgicalreview.org
Requirement One An institutional commitment at the highest levels of the applicant medical staff and the institution’s administration to excellence in the care of the bariatric surgical patient as documented with an ongoing, regularly scheduled, in-service education program in bariatric surgery and utilization of credentialing guidelines for bariatric surgery.
Hospital Administrator Applicant Surgeon(s) Chief Nursing Officer Department Managers for: Bariatric Patient Care Floor(s) Operating Room Imaging Services Emergency Room Intensive Care Unit Bariatric Program Coordinator Physician Extenders involved with the program: Dietitians Physician Assistants Advance Practice Nurses Psychologists Bariatricians Exercise Physiologists Requirement One Inspectors will interview the following during the morning meeting:
Minimum In-service Programs • Bariatric sensitivity training for all staff who interact with the bariatric patient • Training in mobilizing and transferring the morbidly obese patient • Training in recognition of the warning signs of complications from bariatric surgery Remember to document your training with agendas, content and sign-in sheets!
Requirement One Need signed and dated documents • Board certification • General surgery privileges • Bariatric privileges • CME records • Applicant surgeons need 24 Level I CME specific to bariatricsevery three years. • In-service records for staff
Deal Breakersfor Requirement One • Lack of vocal support for the bariatric program by CEO, CNO or administrators during interview • No defined credentialing guidelines for bariatric surgery, separate from standard general surgery privileges • CME requirement not met • No documented in-service program for bariatric team • No regularly scheduled staff educational programs • Attendance not required or documented • Staff unable to verbalize education during interviews
Requirement Two The applicant institution has performed at least 125 bariatric surgical cases in the preceding 12 months and each applicant surgeon has performed at least 125 bariatric cases lifetime with at least 50 cases performed in the last 12 months.
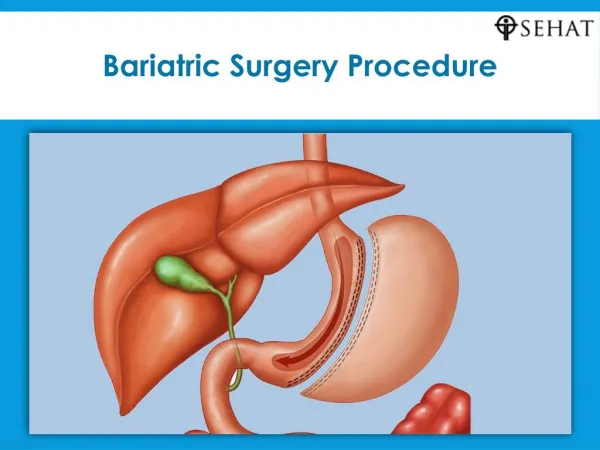
What is a Primary Bariatric Procedure? ASMBS recognizes the following procedures whether performed open or laparoscopic: • Gastric bypass (short or long limb, transected or not transected, banded or not banded) • Vertical banded gastroplasty • Gastric banding • Duodenal switch • Biliopancreaticdiversion • Sleeve gastrectomy
What Other Procedures Count? • Repair of a slipped band • Removal of an eroded band • Repair of the following internal hernias when performed on a post-bariatric surgery patient • Jejuno-jejunostomy • Colonic mesentery • Peterson • Hernias forming around an adhesion
What Doesn’t Count? • Port revisions • Tubing repairs • Gastric band removals (unless replaced during same surgery) • Endoscopic procedures • Exploratory procedures (without revision ) • Repair of the following hernias • Inguinal • Incisional • Umbilical • Port site • Abdominal wall
What is volume for the hospital? Total number of bariatric procedures performed at the applicant institution during the most recent 12 month period. (Includes ALL approved bariatric surgeries at the hospital performed by ALL bariatric surgeons … whether applying for BSCOE or not)!
What is volume for the applicant surgeon? Total number of primary bariatric procedures performed at every facilityduring the most recent 12 month period. • Includes ALL approved bariatric surgeries performed at ALL hospitals • Must be the primary surgeon • NOT the assisting or co-surgeon
Requirement Two • Surgeons may count up to 75 primary cases from their residency or fellowship for their lifetime volume (of 125) • Must include a signed and dated letter from the Chief of the Department of Surgery at that particular hospital verifying the number and type of primary bariatric cases performed and the dates.
Volume Averaging If a facility or surgeon is experiencing a temporary drop in the number of bariatric surgeries being performed, volumes can be averaged over a three-year period. Example: • 1/1/04 - 12/31/04 Volume for facility = 398 • 1/1/05 - 12/31/05 Volume for facility = 250 • 1/1/06 - 12/31/06 Volume for facility = 75 Average for 3 years = 241
Fast-Tracking • If a BSCOE surgeon relocates to a non-BSCOE facility, the non-BSCOE facility may apply with the BSCOE surgeon for Full Approval upon performing 63 cases within the prior six month period. • The BSCOE surgeon must have performed 25 of these 63 cases. • An interim review will be done in 1 year to verify the required volume of 125 cases in a 12-month period have been performed.
Requirement Two It’s all about the data! • Separated and totaled for each surgeon • Re-operations within 30 days • Re-admissions within 30 days • Revisions • Deaths • Transfers HIPAA compliant list for all bariatric surgery procedures during the 12 month period of the review:
Requirement Two • Site inspectors will need access to medical records at the hospital and/or surgeon’s office • Must review the H&P, surgical consent, Operative note and discharge summary • Please tab these documents in un-tabbed paper charts • Print these four documents from an EMR
Deal breakersfor Requirement Two • The institution did not perform 125 bariatric cases in the designated 12 month period • Each applicant surgeon did not perform 125 bariatric cases lifetime and/or 50 bariatric cases in the designated period • Inaccessible medical records • Review of medical records reveals discrepancies • For example, under-reporting mortality, re-operations or re-admissions
Requirement 3 The applicant maintains a designated Medical Director (surgeon) for bariatric surgery who participates in the relevant decision-making administrative meetings of the institution.
Requirement Three Organization of Bariatric Team and Medical Director • Signed agreement and verification of appointment of bariatric surgery medical director • Documentation of the duties and responsibilities for the bariatric medical director and/or co-director
Organization of Bariatric Team and Medical Director (Continued) • A list of bariatric committee members with department representation • Documentation of committee meetings, including: • Dates and times • Minutes • Attendance records • Scheduled dates of future committee meetings
Deal Breakersfor Requirement Three • No bariatric medical director • No qualified bariatric surgeon as medical director • No defined bariatric structure or committee in hospital • No bariatric surgery committee minutes available for review • No regularly scheduled meetings of bariatric committee
Requirement Four The applicant hospital maintains – within 30 minutes of request – a full complement on staff of the various consultative services required for the care of bariatric surgical patients including the immediate availability of an ACLS-qualified physician on site, who can perform patient resuscitations.
Requirement Four Ability to provide responsive critical care to patients • 24 hour/7 day/week ACLS certified physician is the requirement • Need documentation for 30 minuteon site response time of consultant physicians • Anesthesiologist • Cardiologist • Pulmonologist • Intensivist • Endoscopist (or surgeon capable of performing endoscopy) • Interventional Radiologist
Deal Breakersfor Requirement Four • No in-house ACLS qualified physician to perform resuscitations 24/7 and/or no full-time staff 24/7 • Lack of available consultative staff and/or lack of their availability on site within 30minutes • No ventilators, radiologic equipment, or critical care hemodynamic monitoring equipment on-site • No transfer agreement (if applicable)
Requirement Five The applicant maintains a full line of equipment and instruments for the care of bariatric surgical patients including furniture, wheel chairs, operating room tables, beds, radiologic capabilities, surgical instruments and other facilities suitable for morbidly obese patients.
Requirement Five Inspection of equipment and instruments for bariatric surgery patient care Site inspectors will inspect • Operating room • Patient care area(s) • Intensive care unit • Radiology department • Emergency room • Applicant surgeon’s practice
Hospital beds Operating room tables Scales Wheelchairs Stretchers/gurneys Toilet supports Radiologic tables Fluoroscopy CT scan Furniture Exam tables Need documentation of manufacturers’ weight capacities
Floor mounted or supportedwall-mounted toilets are required!
Deal Breakers for Requirement Five • Insufficient equipment or instruments to manage morbidly obese patients • No manufacturer specification sheets • Unsupported wall mounted toilets • Absence of CT or fluoroscopy for UGI series • No transfer devices for the morbidly obese and/or no staff training on the procedure • Staff unaware of weight capacities
Requirement Six The applicant has a bariatric surgeon who spends a significant portion of his or her efforts in the field of bariatric surgery and who has qualified coverage and support for patient care.
Requirement Six • Bariatric call coverage by bariatric surgeon(s) All bariatric surgeons who provide coverage for bariatric patients need to provide the following documentation: • board certification • general surgery and bariatric surgery privileges • a minimum of 24 Level I CME related to bariatric surgery within the last 3 years
Requirement Six Bariatric call coverage by general surgeon(s) All general surgeons who provide coverage for bariatric patients need to provide the following documentation: • board certification • general surgery privileges • a minimum of 12 Level I CME related to bariatric surgery within the last 3 years • assists in the OR for a minimum of 5 non-stapling and/or 10 stapling/anastomoticbariatric procedures
Deal Breakersfor Requirement Six • Lack of board certification for covering bariatric surgeon and/or covering general surgeon • Lack of hospital general surgery and/or bariatric surgery privileges (for bariatric surgeons) • Lack of documentation of required assists for general surgeons • Lack of documentation of 12 Level I CMEs related to bariatric surgery for covering surgeon within lastthree years
Requirement Seven The applicant utilizes clinical pathways and orders that facilitate the standardization of perioperative care for the relevant procedure. In addition, all bariatric procedures are standardized for each surgeon.
What is a Clinical Pathway? A written plan that documents and guides the standardization of care for the uncomplicated patient. Pathways must be formally adopted and implemented at the time of the site inspection.
What is a Clinical Pathway? The path that your patient follows . . . - through the complete continuum of care: • Initial contact with the program • Preoperative • Day of surgery • Immediate postoperative • Post discharge/long-term Format is not as important as content